CMS Final FY26 IPPS and CY26 OPPS Updates: What Hospitals, Physicians, and ASCs Need to Know
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Mike Church, Director, Corazon
Michael Church is a Director at Corazon, offering program development for the Heart, Vascular, Neuroscience, Spine, Orthopedic, and Surgical service lines, offering services in Consulting, Recruitment, Interim Management, Accreditation, and Peer Review.
To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach the author, email michael.church@corazoninc.com
Brief Overview
• The Centers for Medicare & Medicaid Services is reshaping reimbursement across the Inpatient Prospective Payment System for FY26, Outpatient Prospective Payment System and Ambulatory Surgery Center (ASC) payment for CY26, and the Physician Fee Schedule for CY26, using payment updates plus policy levers to push care to lower-cost settings and tighten accountability. Key signals include the inpatient-only list phase-out, broader site-neutral payment, stronger price transparency, and sustained emphasis on quality program performance.
• Inpatient payment updates increase the stakes for coding and Diagnosis-Related Group (DRG) integrity, particularly in cardiovascular services. FY26 includes new cardiovascular DRGs, DRG reassignment and reimbursement shifts, and substantial ICD-10 expansion, alongside the mandatory Transforming Episode Accountability Model (TEAM) bundled payment program for five surgical episodes, making documentation quality, coding audits, and episode-cost management central to protecting reimbursement.
• Outpatient, ASC, and physician rules create near-term opportunity but require deliberate operational planning. Outpatient Prospective Payment System changes include a long-duration conversion factor adjustment tied to prior 340B cuts, expanded ASC Covered Procedure List, and broader non-opioid pain treatment payment, while the Physician Fee Schedule introduces dual conversion factors, an efficiency adjustment for non-time-based services, expanded virtual “direct supervision,” new MIPS (Merit-based Incentive Payment System) Value Pathways, and the upcoming Ambulatory Specialty Model, reinforcing the need for a unified finance, coding, and clinical implementation plan as sites of care shift.
The Centers for Medicare & Medicaid Services (CMS) has finalized its rules for the Inpatient Prospective Payment System (IPPS) for Fiscal Year 2026 (FY26) and the Outpatient Prospective Payment System (OPPS) for Calendar Year 2026 (CY26). These updates will have wide-ranging implications for hospitals, ambulatory surgery centers (ASCs), and physicians, as CMS continues to refine reimbursement structures, quality programs, and site-of-service policies. Together, the rules reflect CMS’s ongoing push toward value-based care, transparency, and cost efficiency.
Inpatient Prospective Payment System (IPPS)
 For FY26, CMS finalized a 2.6% increase in IPPS operating rates for acute care hospitals that meet reporting requirements, including submission of required quality data and “meaningful use” of certified EHR technology. The update is built from a 3.3% market basket* adjustment minus a 0.7% productivity reduction. Hospitals that fail to meet reporting or electronic health record (EHR) standards will see significant reductions to their payments, underscoring CMS’s emphasis on compliance and data-driven care.
For FY26, CMS finalized a 2.6% increase in IPPS operating rates for acute care hospitals that meet reporting requirements, including submission of required quality data and “meaningful use” of certified EHR technology. The update is built from a 3.3% market basket* adjustment minus a 0.7% productivity reduction. Hospitals that fail to meet reporting or electronic health record (EHR) standards will see significant reductions to their payments, underscoring CMS’s emphasis on compliance and data-driven care.
*A CMS market basket is an index measuring the change in price over time of the same mix of goods and services purchased in the base period.
CMS is also continuing its work to rebase the market basket to a 2023 base year. As part of that, the labor-related share used in IPPS payment calculations is being reduced from 67.6% to 66.0%. Because the wage index is applied to the labor-related portion, a smaller labor share means wage index adjustments affect a smaller slice of the payment, which generally reduces funding for hospitals in higher-wage areas relative to the prior methodology.
In parallel, CMS will discontinue the low wage index hospital policy beginning in FY26, as required by a 2024 court ruling. This removes a historical payment boost for certain facilities, but CMS is providing budget-neutral transitional relief that limits the magnitude of the change. Specifically, CMS will cap wage index declines at 9.75%, ensuring affected facilities’ FY26 wage index remains at least 90.25% of their FY24 wage index.
Other finalized IPPS provisions include a $2 billion increase in Disproportionate Share Hospital (DSH) payments, reversing years of decline, and maintenance of the Indirect Medical Education (IME) multiplier at 1.35. CMS also retained the 10% cap on single-year decreases in DRG relative weights. Finally, CMS issued substantial ICD-10 updates, including 487 new billable codes (614 new codes total), 28 deletions, and 28 revisions, largely to improve anatomic site and severity specificity. Examples include more than 100 new codes for non-pressure ulcers and more than 100 new codes tied to adding the body site “flank” within the “Injury, Poisoning, and Certain Other Consequences of External Causes” category.
Quality Programs
CMS’s quality initiatives remain central to the IPPS framework. The Value-Based Purchasing program continues to redistribute 2% of base DRG payments as quality incentives. No new Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey changes were announced for FY26, so the focus remains on evaluating performance from 2025 changes.
The Inpatient Quality Reporting (IQR) program has removed reporting requirements related to Hospital Commitment to Health Equity, Social Determinants of Health (both general screening and screen positive rates), and healthcare provider COVID-19 vaccination coverage, changes which are mirrored in the OPPS and Physician Fee Schedule changes for CY26 as well. IQR also lowered thresholds for hybrid measures (e.g., vital signs and lab tests) to ease reporting burdens. Measures for hip and knee arthroplasty complications and stroke mortality will now include Medicare Advantage patients, among other changes, and it is anticipated these will gradually be applied to the other seven measures starting in FY27.
The Hospital-Acquired Condition program retains its 1% penalty for hospitals in the worst-performing quartile, with the baseline year updated to 2022. Meanwhile, the Hospital Readmissions Reduction Program (HRRP) remains unchanged for FY26, though CMS has signaled significant revisions for FY27, including the addition of Medicare Advantage patients, shorter performance periods, and removal of COVID-related exclusions. Future refinements to the HRRP may also introduce 7- and 14-day readmission cohorts alongside the existing 30-day standard and evaluate Medicare Advantage and Fee-for-Service populations separately. “Leave of absence” billing practices were included in the discussion of readmissions (though no formal rulings related to them), which relates to cases when a readmission is expected but inpatient care is not required during the interim, resulting in only one bill and one DRG payment generated for that scenario, but helping to avoid penalties for unexpected readmissions.
Bundled Payments
A major FY26 change is the start of the Transforming Episode Accountability Model (TEAM), a mandatory bundled payment program for five surgical episodes: joint replacement, hip fracture treatment, spinal fusion, coronary artery bypass graft, and major bowel procedures. Under TEAM, hospitals will receive annual reconciliation comparing actual episode spending to CMS target prices for care delivered from the index surgery through 30 days post discharge; depending on performance, hospitals will either repay CMS or receive a reconciliation payment. CMS has already distributed 2026 target prices to participating facilities. Hospitals can choose among risk tracks to manage financial exposure, and safety-net and rural facilities may qualify for reduced downside risk.
DRG Changes
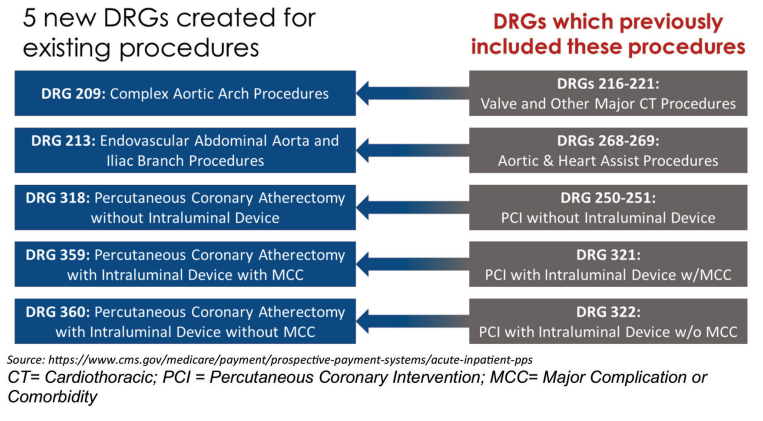
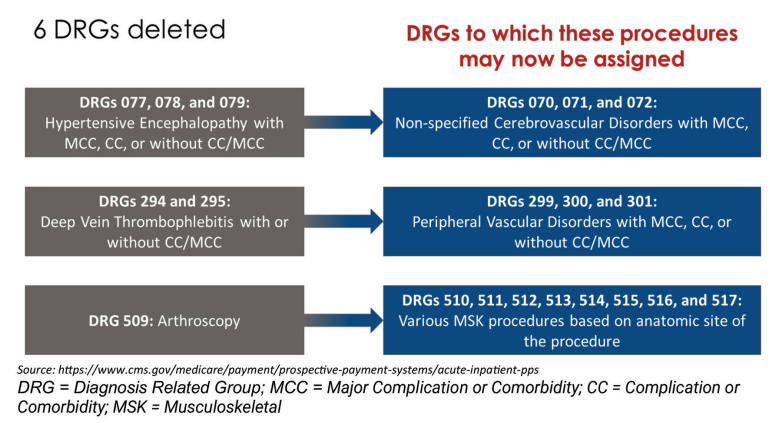
CMS created five new DRGs to better reflect the higher resource costs associated with certain complex procedures, and deleted six DRGs, reassigning those cases into broader DRG categories. All five new DRGs relate to cardiovascular procedures, specifically selected aortic procedures and coronary atherectomy procedures. Figures A and B show where these cases were historically assigned (gray boxes) and where they will be assigned beginning in FY26 (blue boxes). CMS has also issued additional coding guidelines to support implementation of these DRG changes.
DRG Reimbursement
When reviewing FY26 inpatient reimbursement updates, base reimbursement increased across all coronary artery bypass graft (CABG) and cardiac valve surgery DRGs, which is relatively uncommon. For surgical valve DRGs, CMS applied a monotonicity correction† to DRGs 217 and 218 to ensure the higher-acuity DRG does not pay less than the lower-acuity DRG. In this case, DRG 217 represents patients with complications and comorbidities, while DRG 218 represents patients without them. Cardiac surgery programs often have opportunities to improve coding accuracy and fully capture complications and comorbidities, which can materially affect reimbursement. As reimbursement for patients without complications and comorbidities catches up to payments for patients with complications and comorbidities, coding audits and strong documentation become even more important to support accurate coding and billing.
† “Monotonicity correction” refers to methods used to adjust data, functions, or numerical schemes to ensure they maintain a consistent, non-reversing trend (either always increasing or always decreasing).
Even more uncommon, both DRGs 266 and 267 (transcatheter aortic valve replacement, TAVR) also increased. As TAVR has become more prevalent and techniques have advanced, payment rates for these DRGs have generally trended downward, so this increase will be welcome given the narrow margins many TAVR programs face.
DRGs 023 and 024 for craniotomies with device (including stroke thrombectomy and neurointervention procedures) increased again in FY26 as this therapy continues to gain recognition as the standard of care for a growing stroke population. Several peripheral vascular DRGs, both catheter-based and surgical, also increased, by as much as 15% in FY26. Peripheral vascular disease remains highly underdiagnosed and undertreated, creating opportunity, particularly for organizations already offering coronary intervention services.
With respect to reimbursement for the new DRGs (Figure A), DRG 209 reimburses at a higher rate than the previously assigned DRGs. Reimbursement for DRG 213 falls between reimbursement for the previously assigned DRGs (268 and 269), so coding accuracy remains important to ensure appropriate DRG assignment and reimbursement. The new atherectomy DRGs (318, 359, and 360) are also reimbursed at a rate $2,000 to $7,000 higher than the previously assigned DRGs.
Outpatient Prospective Payment System (OPPS)
For CY26, CMS finalized a 2.6% payment update for hospital outpatient departments (HOPDs) and ambulatory surgery centers (ASCs), translating to an estimated $101 billion in HOPD payments and $9.2 billion for ASCs.
A major driver within the OPPS conversion factor is a continued clawback of $7.8 billion in overpayments from 2018–2022, implemented as a -0.5% adjustment that CMS expects could last up to 16 years. This traces back to CMS’s 2018 reduction in OPPS reimbursement for 340B drugs‡, which was reversed in 2023 after the U.S. Supreme Court found the 2018 cuts were not consistent with CMS authority. CMS then issued a one-time lump sum payment in 2023 to repay the underpaid drug amounts. However, because the original 2018 policy was implemented in a budget-neutral way, that lump sum did not account for the corresponding higher payments for non-drug items and services during the same period. CMS is addressing that mismatch by applying the conversion factor adjustment starting in CY26. CMS proposed increasing the clawback amount for CY26 but did not finalize that increase, though it remains an option for CY27 and beyond.
‡ “340B drugs”: Section 340B of the Public Health Service Act requires pharmaceutical manufacturers participating in Medicaid to sell outpatient drugs at discounted prices to health care organizations that care for many uninsured and low-income patients.
CMS is also expanding site-neutral payment policies by applying physician fee schedule-equivalent rates to drug administration services in certain off-campus provider-based departments. CMS estimates this will save up to $290 million in CY26 and $11 billion over the next decade, with some savings also flowing to beneficiaries.
Another major update is the long-anticipated phase-out of the inpatient-only (IPO) list, beginning in CY26 with a three-year transition. In the first year, 285 codes (primarily musculoskeletal procedures) will be removed, giving physicians greater discretion in selecting the most appropriate site of care. CMS noted these procedures can still be performed in the inpatient setting and that the intent is to improve appropriateness and patient outcomes.
Additional OPPS policies include reclassifying skin substitutes as incident-to supplies, conducting the first drug acquisition cost survey since 2005, and strengthening hospital price transparency requirements. Enforcement of certain price transparency requirements (such as listing actual dollar amounts whenever possible and disclosing additional amounts when possible) has been delayed until April 1, 2026. CMS also expanded reimbursement for non-opioid pain treatments, adding five drugs and thirteen devices eligible for separate payment in both HOPD and ASC settings to support efforts to reduce opioid-use disorder risk.
Ambulatory Surgery Centers (ASCs)
ASCs will receive the same 2.6% payment update as hospital outpatient departments. A major policy change for CY26 is a significant expansion of the ASC Covered Procedure List, which now includes electrophysiology ablations, percutaneous coronary intervention (PCI) procedures, spinal fusions, and vascular embolizations. In addition, 271 codes removed from the inpatient-only list have been added to the ASC list, reinforcing CMS’s direction of moving more complex services into outpatient settings.
CMS made these expansions, at least in part, by revising the ASC’s general exclusions and moving five long-standing criteria into a new section titled “nonbinding physician considerations for patient safety”:
1. Procedures which generally result in extensive blood loss;
2. Procedures which require major or prolonged invasion of body cavities;
3. Procedures which directly involve major blood vessels;
4. Procedures which are generally emergent or life-threatening in nature;
5. Procedures which commonly require systemic thrombolytic therapy.
Reclassifying these criteria supports the broader phase-out of the IPO list and emphasizes physician discretion based on patient needs and safety.
From a financial standpoint, ASC reimbursement remains roughly 30% lower than HOPD, but this is typically offset by a similar reduction in ASC operating costs, resulting in comparable margins. Notably, reimbursement for approved EP ablation codes in ASCs is much closer to the HOPD reimbursement rate than many other procedures. Organizations should assess their own economics, but this could be an opportunity for ASCs beginning EP ablation services, since reimbursement may be relatively more favorable in CY26 than in future years. That timing may help offset startup costs, including new equipment, particularly as outpatient ablation volumes continue to grow.
Physician Fee Schedule (PFS)
For CY26, CMS is introducing two separate conversion factors: a 3.77% increase for Qualifying Alternative Payment Model (APM) participants and a 3.26% increase for non-QP providers. These updates reflect statutory changes from the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) and the One Big Beautiful Bill Act, along with a 0.49% increase tied to changes in work Relative Value Units (RVUs). CMS also finalized a -2.5% efficiency adjustment to non-time-based services, and updated the practice expense methodology to better reflect indirect costs in office-based settings. In addition, CMS permanently expanded the definition of direct supervision to include real-time virtual communication, applicable across all care settings, not only physician practices.
Within the Medicare Shared Savings Program, CMS reduced the amount of time an Accountable Care Organization (ACO) can remain in a one-sided risk track§ and adjusted the number of beneficiaries assigned in each benchmark year, effective in 2027. CMS also created new MIPS (Merit-based Incentive Payment System) Value Pathways for six services:
1. Diagnostic Radiology
2. Interventional Radiology
3. Neuropsychology
4. Pathology
5. Podiatry
6. Vascular Surgery
Looking ahead, CMS finalized the Ambulatory Specialty Model (ASM) for launch in 2027. This mandatory model will apply to specialists caring for Medicare patients with heart failure or low back pain, using the MIPS Value Pathways framework to assess quality, cost, and patient engagement. Incentives will range from ±9% initially to ±12% by the program’s conclusion in 2031. While the program has been announced, CMS is expected to release additional details, and potentially further changes, before implementation.
Conclusion
The FY26 IPPS and CY26 OPPS rules represent a significant evolution in Medicare reimbursement, with changes spanning inpatient, outpatient, ASC, and physician payment systems. Hospitals will need to adapt to new coding structures, quality reporting requirements, and bundled payment models, while ASCs and physicians face expanded opportunities and responsibilities in outpatient care. With the IPO list phasing out, site-neutral payments expanding, and transparency rules tightening, a unified strategy to understand the impact of each rule will become even more vital as sites of care shift and clinical pathways evolve.