Conversations in Cardiology: Pectus Excavatum and Coronary Compression in the Elderly
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Mort Kern with contributions from Steve Goldberg, Las Cruces, New Mexico; Dean Kereiakes, Cincinnati, Ohio; Mike Ragosta, Charlottesville, Virginia; Ken Rosenfield, Boston, Massachusetts; Carl Tommaso, Chicago, Illinois.
Morton J. Kern, MD, MSCAI, FACC, FAHA
Clinical Editor; Interventional Cardiologist, Long Beach VA Medical Center, Long Beach, California; Professor of Medicine, University of California, Irvine Medical Center, Orange, California
Disclosures: Dr. Morton Kern reports he is a consultant for Abiomed, Abbott Vascular, Philips, ACIST Medical, and Opsens Inc.
Dr. Kern can be contacted at mortonkern2007@gmail.com
On X @MortonKern
Pectus excavatum is a structural deformity of the anterior thoracic wall in which the sternum and rib cage produce a caved-in or sunken configuration of the chest. It can be congenital at birth or develop after puberty. Pectus excavatum can impair cardiac and respiratory function and cause pain in the chest and back. Some patients report difficulty with strenuous activity due to the restricted lung capacity. Pectus excavatum is often associated with other malformations, including scoliosis, kyphosis, and connective tissue disorders such as Marfan syndrome. Surgery may not alleviate chest pain, but it can correct the sunken chest and improve the patient’s quality of life.
The Clinical Dilemma
Ischemia in nonagenarians (90-year-olds) can be a challenge to sort out. Dr. Mike Ragosta from Charlottesville, Virginia, writes about a difficult case. Here it is.
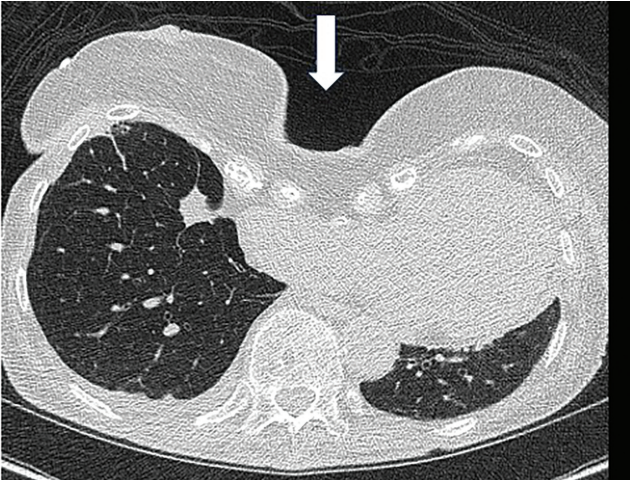
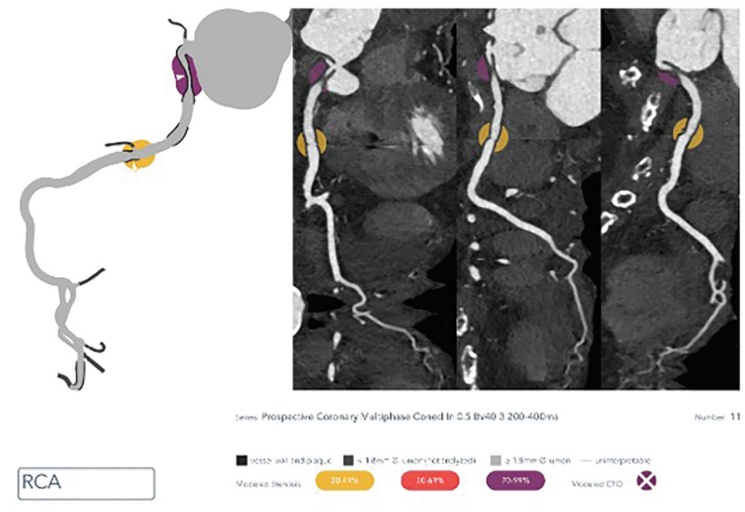
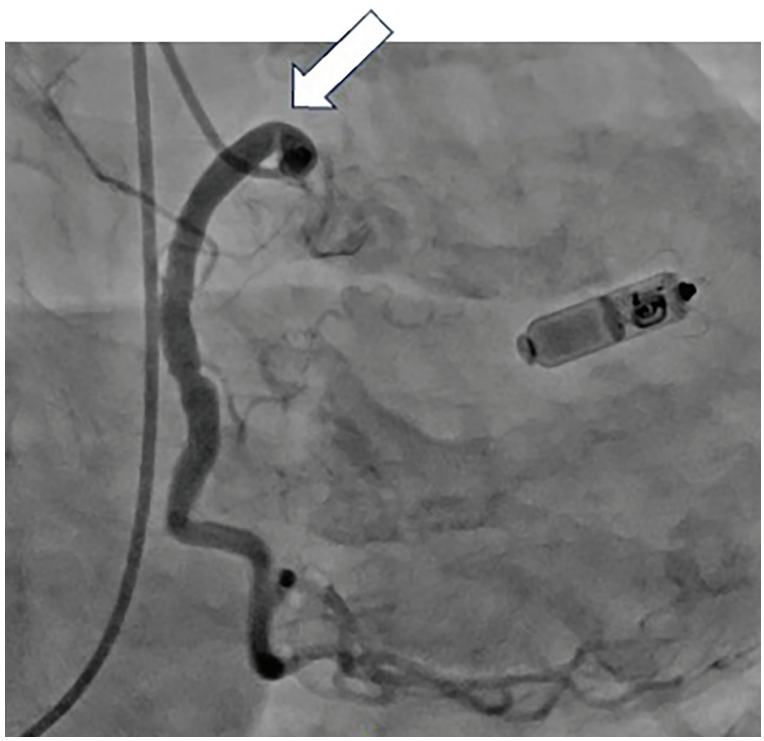
“I had an interesting case recently [where] I would love to get an opinion regarding management. This patient was a robust and healthy 92-year-old person with onset of angina about a year ago. Angina has gotten progressively worse and the patient can no longer do any exertion without angina. The past medical history is significant for only osteoporosis and arthritis. The pectus excavatum on exam and radiologically is impressive (see Figures 1-3). The primary physician went directly to a coronary CTA [computed tomography angiography] which showed that the right atrium and the RCA [right coronary artery] are compressed by the pectus deformity. I did a coronary angiogram and there appears to be a prominent kink in the proximal RCA at the site of the external compression. It was difficult to see as the only view that showed it was an AP [anteroposterior] with some caudal angulation.
I have never seen this before and wondered if the group has ideas about treatment. Stenting seems like a bad idea, as the stent will either compress or fracture from fatigue. I would love to hear thoughts about this.”
![]() Mort Kern, Long Beach, California: Mike, fascinating case. In a 92-year-old with pectus excavcatum and a severe, very proximal RCA stenosis, it is likely an atherosclerotic routine culprit lesion that has probably been there for a while. Several points come to mind in addressing this senior. The pectus is not new, and I doubt it has anything to do with the RCA lesion. The proximal RCA location is amenable to stenting and is unlikely be impacted by the forces of the heart and pectus. Lastly, medical management of angina works most of the time. After maxing out the medications, I would discuss a stent with the patient.
Mort Kern, Long Beach, California: Mike, fascinating case. In a 92-year-old with pectus excavcatum and a severe, very proximal RCA stenosis, it is likely an atherosclerotic routine culprit lesion that has probably been there for a while. Several points come to mind in addressing this senior. The pectus is not new, and I doubt it has anything to do with the RCA lesion. The proximal RCA location is amenable to stenting and is unlikely be impacted by the forces of the heart and pectus. Lastly, medical management of angina works most of the time. After maxing out the medications, I would discuss a stent with the patient.
![]() Ken Rosenfield, Boston, Massachusetts: Agree with Mort. I would approach this elderly patient as having typical angina with an RCA stenosis. The pectus is quite severe, but I would not assume it the cause of the stenosis.
Ken Rosenfield, Boston, Massachusetts: Agree with Mort. I would approach this elderly patient as having typical angina with an RCA stenosis. The pectus is quite severe, but I would not assume it the cause of the stenosis.
![]() Dean Kereiakes, Cincinnati, Ohio: Agree with Mort and Kenny. True, true, and unrelated. Fix the RCA.
Dean Kereiakes, Cincinnati, Ohio: Agree with Mort and Kenny. True, true, and unrelated. Fix the RCA.
![]() Steve Goldberg, Las Cruces, New Mexico: I would think intravascular ultrasound (IVUS) could resolve the issue. Is this typical atherosclerosis or external compression? If it’s compression, I would rethink stenting.
Steve Goldberg, Las Cruces, New Mexico: I would think intravascular ultrasound (IVUS) could resolve the issue. Is this typical atherosclerosis or external compression? If it’s compression, I would rethink stenting.
 Carl Tommaso, Chicago, Illinois: Pectus has been present all her life. Symptoms appeared only recently. If one can’t control symptoms with medical therapy, I would not hesitate to fix it.
Carl Tommaso, Chicago, Illinois: Pectus has been present all her life. Symptoms appeared only recently. If one can’t control symptoms with medical therapy, I would not hesitate to fix it.
![]() Anonymous Colleague: Documented cases of RCA compression due to pectus excavatum are rare, but well-described in the literature. The treatment is surgical repair of the pectus.
Anonymous Colleague: Documented cases of RCA compression due to pectus excavatum are rare, but well-described in the literature. The treatment is surgical repair of the pectus.
Here are some case examples. Benedetti and colleagues report the case of a 74-year-old woman with exertional angina and pectus excavatum.1 Evaluation identified that severe pectus excavatum had caused a small right coronary ostium to be compressed by the chest wall.
While angina was similarly the complaint of Mike Ragosta’s patient, there are other cases of sudden cardiac death, such as the case of a 44-year-old male with syncope triggered by ventricular fibrillation.2 Imaging revealed a severe chest wall deformity causing tight stenosis at the origin of the RCA due to external mechanical compression.
Spentzou et al report a 16-year-old with severe pectus excavatum and epicardial pacing leads who experienced exercise-induced ventricular tachycardia.3 A CT angiogram showed the atrial pacing wire was forced against the RCA by the sternal indentation, leading to arterial compression.
Pectus excavatum in a 56-year-old woman caused chest pain specifically when lying on her right side.4 Angiography confirmed proximal compression of the RCA only in that specific lateral position, which resolved after surgical chest wall repair.
It is noteworthy that while right ventricular compression is common, displacement or compression of the RCA is a rare but has been documented in severe cases. The mechanisms of ischemia may include:
- Mechanical Impingement: Direct pressure from the depressed sternum on the RCA origin or proximal segment.
- Postural Compression: Compression that only occurs during specific body movements or positions (e.g., lying on the right side).
- Secondary Obstruction: Internal hardware (like pacing leads) being pushed into the artery by the chest wall deformity.
The primary goal of treatment is to remove the external pressure by reshaping the chest wall. Methods include the Nuss procedure (minimally invasive), the most used approach.5 Surgeons insert one or more curved metal bars behind the sternum to lift it away from the heart. Studies show a 95% success rate in relieving cardiac compression. Patients typically see immediate improvement in heart function and a resolution of exertional symptoms. Alternatively, the Ravitch procedure (open surgery) can be used and involves removing deformed rib cartilage and repositioning the sternum.5 It is often reserved for older adults with more rigid chest walls or complex deformities. Combined procedures have been proposed for patients with existing heart damage or other cardiac defects. Surgeons may perform a “single stage” repair that combines the chest wall correction with coronary artery bypass grafting (CABG).5
Stenting is rarely utilized for this specific condition because of external mechanical pressure rather than internal arterial disease.
In sum, in contrast to Mort’s view, external compression by pectus is a real entity. I don’t know enough about this patient to say if the RCA lesion is routine atherosclerosis or mechanical. Obviously, further evaluation by reviewing the imaging with an experienced radiologist is key. Looking over traditional risk factors and stress testing are an absolute necessity. An IVUS would be helpful for determining compression versus atherosclerosis. Also, pectus compression is often positional. If an expert radiologist says symptoms are due to pectus excavatum, I’d pay attention and think twice.
I’m a contrarian in this conversation. The secret to being a contrarian is to understand what you’re talking about. I saw a case like this in a young man 30 years ago. One case 3 decades ago hardly designates one an expert, and I’m not.
![]() Mike Ragosta, Charlottesville, Virginia: Thanks all for the input. The CT folks are pretty convinced the lesion is from external compression and hypothesize that, while she has had it her whole life, aging and progressive kyphosis led to compression. I agree with meds first and then if ongoing symptoms, will bring her back and IVUS. If its atherosclerosis, then a big fat stent should fix it.
Mike Ragosta, Charlottesville, Virginia: Thanks all for the input. The CT folks are pretty convinced the lesion is from external compression and hypothesize that, while she has had it her whole life, aging and progressive kyphosis led to compression. I agree with meds first and then if ongoing symptoms, will bring her back and IVUS. If its atherosclerosis, then a big fat stent should fix it.
The Bottom Line
Whether this 92-year-old patient’s symptoms are due to RCA compression or to a separate process of atherosclerotic narrowing amenable to simple stenting remains entirely conjecture. Given the patient’s age, I favor the latter scenario. Thanks, Dr. Ragosta, (and my expert colleagues), and keep us informed.
References
1. Benedetti A, Roba M, Castaldi G, et al. Intravascular ultrasound diagnosis of right coronary artery compression in patient with pectus excavatum. JACC Cardiovasc Interv. 2023 Mar 27; 16(6): 734-736. doi:10.1016/j.jcin.2023.01.377
2. Labarta-Bello C, Ugueto-Rodrigo C, Martín-Arena MA, et al. Severe pectus excavatum: unusual cause of sudden cardiac death linked to a novel genetic variant. JACC Case Rep. 2026 Jan 28; 31(4): 105943. doi:10.1016/j.jaccas.2025.105943
3. Spentzou G, Atkin K, Konstantinov IE, Pflaumer A. Coronary artery compression by pectus excavatum and an epicardial pacing lead. Eur Heart J. 2021 Feb 21; 42(8): 874. doi:10.1093/eurheartj/ehaa1041
4. Heitzer TA, Wollschläger H. Images in cardiovascular medicine. Pectus excavatum with inferior ischemia in right lateral position. Circulation. 1998 Aug 11; 98(6): 605-606. doi:10.1161/01.cir.98.6.605
5. Stephens EH, Dearani JA, Jaroszewski DE. Pectus excavatum in cardiac surgery patients. Ann Thorac Surg. 2023 May; 115(5): 1312-1321. doi:10.1016/j.athoracsur.2023.01.040