Outcomes in Patients With and Without Chronic Limb-Threatening Ischemia: A Systematic Literature Review on Atherectomy for Peripheral Interventions
Abstract
Objectives: To comprehensively summarize the evidence quality and clinical outcomes following peripheral atherectomy in patients with and without chronic limb-threatening ischemia (CLTI). Methods: A PRISMA- and MOOSE-compliant systematic literature review (Medline, Embase, PubMed) identified original research published through November 2024 evaluating atherectomy for peripheral endovascular revascularization. Randomized and non-randomized controlled studies, prospective and retrospective studies, and claims analyses were included. Primary outcomes were distal embolization, provisional stenting and 12-month primary patency, target lesion revascularization, major amputation, and all-cause mortality across 4 patient cohorts based on CLTI prevalence. Results: Thirteen papers reported on outcomes in claudicants and 25 reported on CLTI. Mixed cohorts of >0% to <50% CLTI were reported in 97 papers and ≥50% to <100% CLTI in 51. Most designs were observational (89.0%) and 8.3% were randomized; 41.4% were prospective. Effectiveness was generally consistent across CLTI prevalence; patency was 68.4% in claudicants, 78.4% in the >0% to <50% CLTI cohort, 76.0% in the ≥50% to <100% CLTI cohort, and 82.8% in patients with CLTI. Major amputation and mortality increased with CLTI prevalence: 0.6%, 0.9%, 4.1%, and 5.8% for amputation and 0.3%, 2.1%, 6.1%, and 5.0% for mortality, respectively. Distal embolization and provisional stenting rates were low, particularly in the 100% CLTI cohort (1.6% and 4.6%, respectively). Discussion: Atherectomy provided consistent results in both CLTI and claudication, with favorable safety outcomes compared to previously published reports of other endovascular techniques. Conclusion: The body of evidence supports atherectomy as a vessel preparation tool in endovascular procedures across a range of disease severity.
J CRIT LIMB ISCHEM 2026:6(1):E16-E34. doi: 10.25270/jcli/CLIG-2600001
Key words: atherectomy, chronic limb-threatening ischemia, claudication, critical limb ischemia, peripheral arterial disease
Chronic limb-threatening ischemia (CLTI) is associated with high morbidity and mortality, with reported 1-year amputation and mortality rates of 22% in patients not undergoing revascularization.1 Prompt revascularization is therefore critical both to alleviate symptoms and reduce the risk of amputation.
While global guidelines support revascularization in patients with CLTI,2-4 the most safe and effective approach remains unclear. For the endovascular approach, angioplasty and stenting can improve amputation-free survival in patients with CLTI compared to surgical bypass.5 However, the effectiveness of endovascular intervention may be challenged by the presence of calcification,6 which is common in patients with CLTI.7,8 Complex lesions, including calcified lesions and total occlusions, are also more prone to residual stenosis and the need for provisional stenting in order to achieve optimal periprocedural outcomes.9,10
Vessel preparation with atherectomy may improve outcomes in complex lesions by reducing plaque burden and the impact of barotrauma with angioplasty alone, favorably impacting vessel compliance, enlarging the treated lumen, and improving vessel wall apposition of drug-coated devices.11 In turn, reduced residual stenosis lessens the need for permanent stenting and thereby preserves future treatment options,12-14 which is particularly important in patients with CLTI at high risk for recurrence. In a meta-analysis of 10 randomized trials and observational studies evaluating atherectomy prior to balloon angioplasty for the treatment of infrapopliteal lesions, the use of atherectomy resulted in significantly lower rates of clinically driven target lesion revascularization (TLR) and major amputation compared to angioplasty alone.15 However, more data is needed on the use of atherectomy in patients with CLTI, particularly real-world evidence that reflects a diverse range of patients, lesions, and operator experience.16
The objective of this systematic literature review and meta-analysis was to provide a comprehensive overview of the literature evaluating atherectomy in patients with and without CLTI, including both the quality of the compiled evidence and 12-month clinical outcomes.
Methods
Eligibility criteria, information sources, and search strategy
A full description of the methods has been previously reported.17 A PRISMA- and MOOSE-compliant18,19 systematic literature review of Medline, Embase, and PubMed identified 322 original research articles published through November 2024 evaluating atherectomy (with or without adjunctive therapies) for percutaneous revascularization of de novo or restenotic lesions in infrainguinal, native, peripheral arteries. Randomized and non-randomized controlled studies, single-arm prospective studies, retrospective series, database/claims analyses, and case reports were included in the search. Review articles, letters, conference abstracts, books, trade journals, non-English language, and non-human interventions were excluded. Full-text articles meeting the inclusion criteria were each read by 2 reviewers and discrepancies were resolved by consensus. Original authors were not contacted.
Assessments and definitions
The predetermined primary outcomes assessed were the 12-month rates of primary patency, TLR, major amputation, and all-cause mortality, as well as clinically significant distal embolization and the use of provisional (unplanned) stents. For this analysis, primary patency was defined as angiographic or duplex ultrasound patency (<50% angiographic stenosis or peak systolic velocity ratio of ≤2.4) and/or by the absence of TLR. CLTI at baseline was classified as Rutherford classification categories (RCC) 4 through 6, or as designated in the original study. Severe calcification was defined according to the individual study reports, or as Peripheral Arterial Calcium Scoring System grade 4 when available. Distal embolization was considered clinically significant if it was identified by the original investigators or required intervention; instances of filter capture not necessitating intervention were excluded from the meta-analysis. Provisional stenting was defined as unplanned stenting for suboptimal results (eg, residual stenosis >30%, flow-limiting dissection, or perforation). Studies that did not define the reasons for stenting were excluded from the provisional stenting analysis. All additional data points were captured according to the definitions provided in the primary sources. Use of adjunctive therapies such as uncoated angioplasty balloons, drug-coated balloons (DCBs), and planned stents was captured and has been previously reported.17
In a post-hoc secondary analysis, outcomes were stratified based on the prevalence of CLTI in the published study cohorts. Four cohorts were assessed: (1) papers evaluating 100% claudicant patients; (2) papers evaluating 100% CLTI patients; (3) papers evaluating mixed cohorts including >0% to <50% CLTI patients; and (4) papers evaluating mixed cohorts including ≥50% to <100% CLTI patients.
Statistics
Baseline demographic, lesion, and procedural characteristics were evaluated with descriptive statistics. Meta-analyses, case reports, redundant studies, and those not reporting the outcomes of interest were excluded from the meta-analysis. Database/claims analyses on overlapping patient cohorts were excluded from the quantitative meta-analysis to prevent redundant reporting; in those cases, the most complete and current analysis was selected. The meta-analysis of predefined outcomes used a random effects model.20 Kaplan-Meier survival estimates or cumulative incidences were treated as proportions by multiplying the survival estimate (or cumulative incidence) by the sample size to approximate the number of events, possibly resulting in a non-integer value. When at least one value for the number of events contained a non-integer value, normal approximation confidence intervals were used. Heterogeneity was assessed using Cochran’s Q-statistic and I2 test; heterogeneity was deemed “substantial” for I2 values ≥50% and “considerable” for I2 values ≥75%.21 Risk of bias testing has been previously reported for the primary analysis.17 Tests of statistical significance were not employed due to inherent heterogeneity of the data. All analyses were performed using R version 4.4.0 and the meta package version 7.0-0.20,22
Ethical statement
Ethical approval was not required for this systematic review and meta-analysis of published literature. Drs Carr, Langhoff, and Secemsky had full access to all the data in the study and take responsibility for the integrity of the analysis. The authors received no funding from the sponsor to write this article.
Results
The primary results of this systematic review and meta-analysis have been previously reported.17 A total of 322 papers reporting on atherectomy outcomes and meeting the inclusion criteria were included in the overall systematic review. Among those, 180 unique papers were included in the CLTI sub-analysis. These included 13 papers evaluating 100% claudicant patients, 25 papers evaluating 100% CLTI patients, 97 papers evaluating mixed cohorts including >0% to <50% CLTI patients, and 51 papers evaluating mixed cohorts including ≥50% to <100% CLTI patients. Individual counts sum to 186 due to multiple subgroups in 6 papers. The papers included in each cohort are listed in Appendix 1. Excluded from the 322 papers in the overall systematic review17 were 12 meta-analyses, 48 case reports, 30 redundant papers (eg, sequential follow-up or subgroup results from an already reported study), 13 claims analyses with overlapping cohorts, and 39 papers not reporting the proportion of CLTI patients enrolled.
Atherectomy types among the 180 papers included in the CLTI sub-analysis consisted of 39.2% directional (71 papers), 21.5% rotational (39 papers), 17.1% laser (31 papers), 8.3% orbital (15 papers), and 13.8% mixed classes (25 papers). Counts sum to 181 due to multiple subgroups reported in one paper.23 Study designs were 15 papers of randomized controlled trials (8.3%), 161 observational studies (89.0%), and 5 claims analyses (2.8%). One paper included both randomized and observational components.24 Seventy-four studies were prospective (41.1%). Adjunctive therapies following atherectomy were used in 91.6% (153/167) of studies reporting that information, most commonly uncoated balloon angioplasty (40.6%), DCBs (43.8%), or bare metal stents (10.0%).
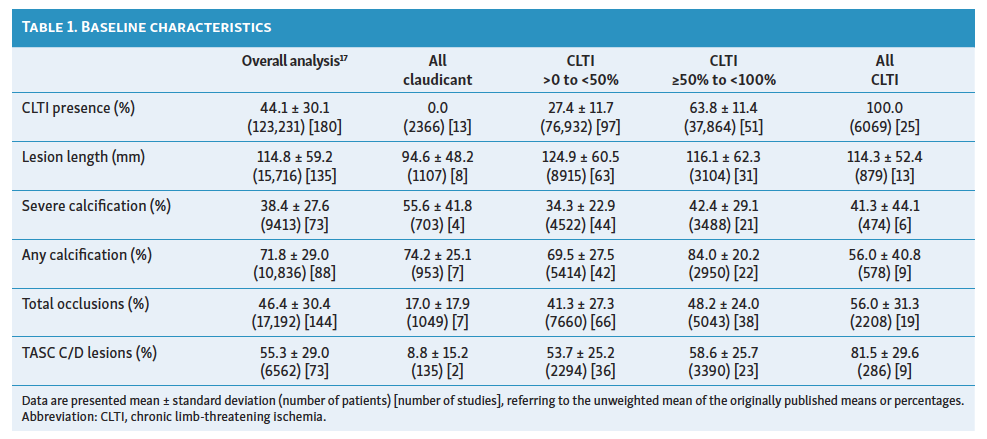
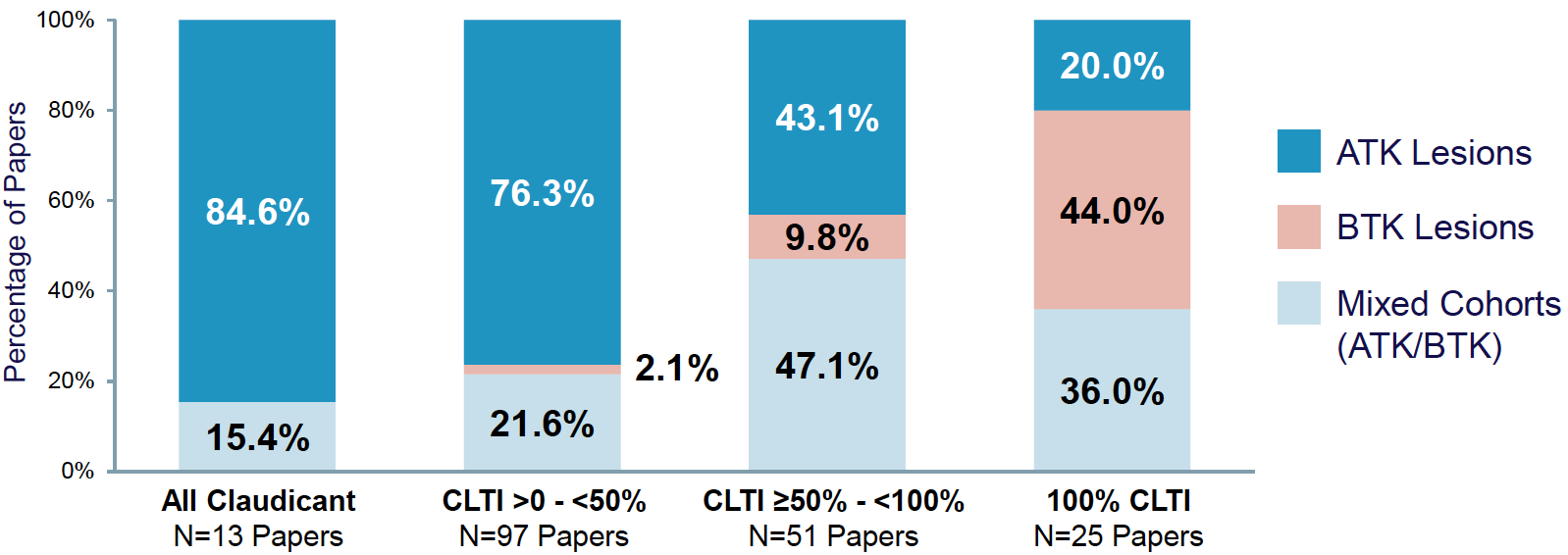
Baseline lesion and disease severity characteristics are shown in Table 1. Most studies evaluated mixed populations, including both claudicant and CLTI cohorts. In the CLTI >0% to <50% cohort, an average of 27.4 ± 11.7% of patients presented with CLTI vs 63.8 ± 11.4% in the CLTI ≥50% to <100% cohort. Lesion characteristics were relatively similar across cohorts, with the exceptions of shorter lesions in the 100% claudicant cohort (94.6 ± 48.2 mm), higher average calcification in the CLTI ≥50% to <100% cohort (84.0 ± 20.2%), higher severe calcification in the claudicant cohort (55.6 ± 41.8%), and a greater prevalence of total occlusions (56.0±31.3%) and TASC C/D lesions (81.5±29.6%) in the 100% CLTI cohort. Figure 1 shows the proportion of above-the-knee (ATK) disease and below-the-knee (BTK) disease across the 4 cohorts evaluated. In the 100% CLTI cohort, 20.0% of papers included only ATK lesions, 44.0% included only BTK lesions, and 36.0% enrolled patients with either ATK or BTK lesions. In the 100% claudicant cohort, 84.6% of studies enrolled patients with ATK disease while 15.4% enrolled mixed cohorts of either ATK or BTK disease.
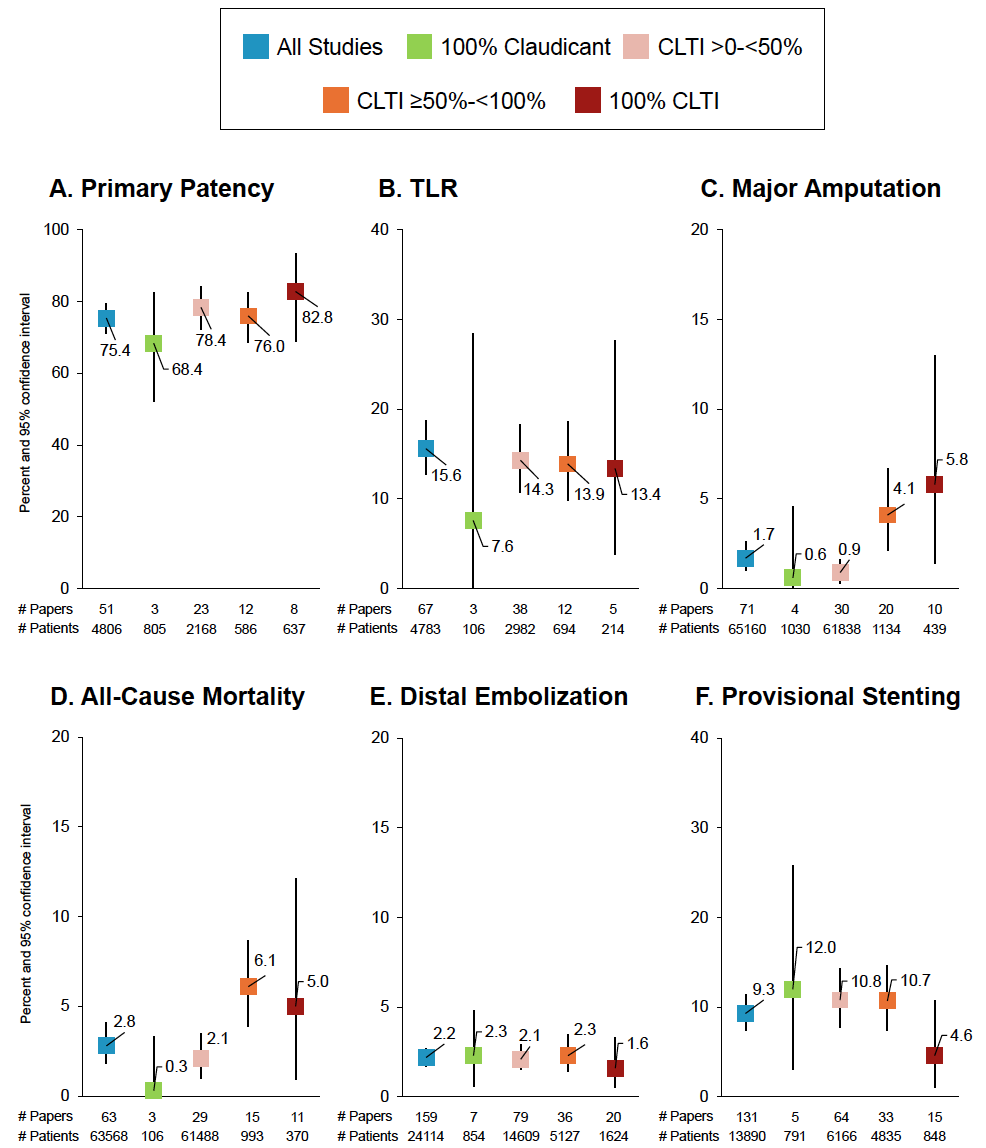
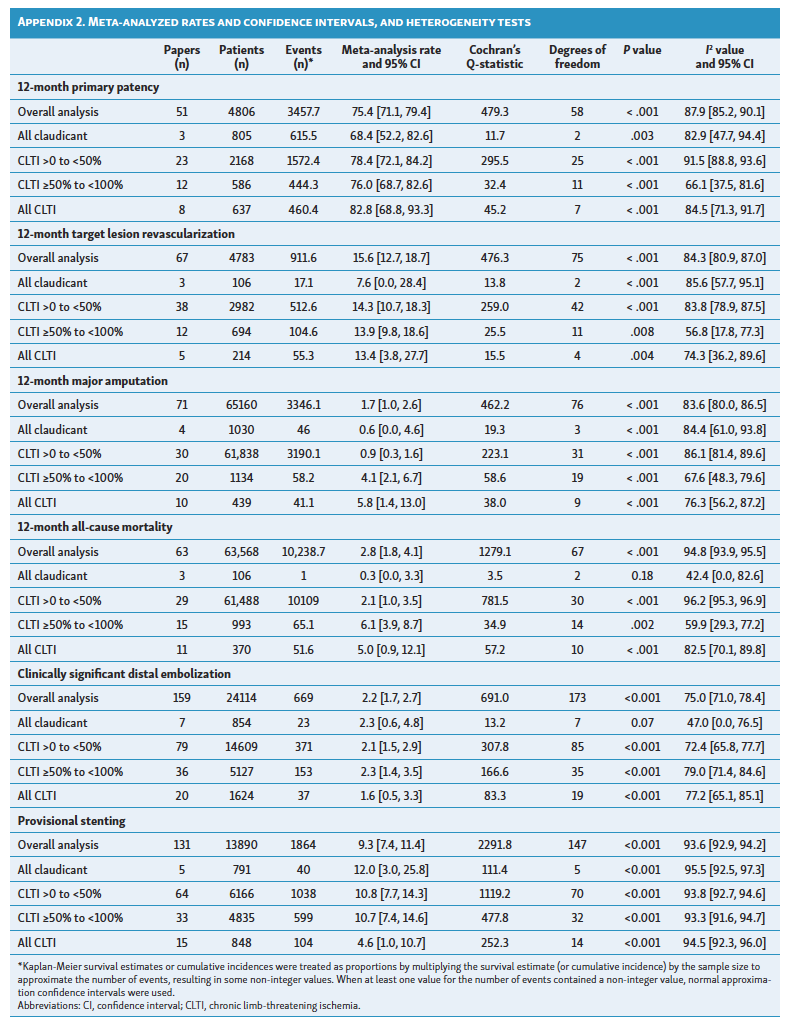
Twelve-month and periprocedural outcomes are shown in Figure 2 and Appendix 2. Overall results have been previously reported.17 Primary patency was 75.4% (95% confidence interval [CI] 71.1-79.4%) overall, based on the total meta-analysis of 51 papers comprising 4806 patients.17 Patency was 68.4% (95% CI 52.2-82.6%) for the 3 papers evaluating 100% claudicant populations. Individual rates were 54.3% in the CELLO laser atherectomy study,25 68.8% the DEFINITIVE AR severely calcified cohort evaluating directional atherectomy followed by DCB,24 and 78.0% in the DEFINITIVE LE study of directional atherectomy followed by standard angioplasty.26 Patency rates trended higher for cohorts with greater proportions of CLTI patients, with 82.8% patency (95% CI 68.8-93.3%) in the 8 papers evaluating 100% CLTI cohorts. TLR was 15.6% overall (95% CI 12.7-18.7%) in the meta-analysis of 67 papers with 4783 patients. TLR was 7.6% (95% CI 0-28.4%) in the 3 papers presenting on 100% claudicant cohorts,24,25,27 but similar across cohorts with increasing proportions of CLTI patients (14.3%, 13.9%, and 13.4%, Figure 2B). The meta-analyzed major amputation rate was 1.7% overall (95% CI 1.0-2.6%) with rates generally increasing with increasing proportions of CLTI patients in the population, from 0.6% in the 100% claudicant cohort (95% CI 0.0-4.6%) to 5.8% in the 100% CLTI cohort (95% CI 1.4-13.0%). Similarly, 12-month all-cause mortality was 2.8% overall (95% CI 1.8-4.1%), increasing from 0.3% (95% CI 0.0-3.3%) to 5.0% (95% CI 0.9-12.1%) in the 100% claudicant and 100% CLTI cohorts, respectively. The rates of clinically significant distal embolization were similar across cohorts and low overall (2.2%, 95% CI 1.7-2.7%). Provisional stenting was 9.3% overall (95% CI 7.4-11.4%) across 131 studies with 13,890 patients; numerically lower rates were observed in the 100% CLTI cohort (4.6%, 95% CI 1.0-10.7%). Considerable or substantial heterogeneity was observed for most meta-analyzed rates (Appendix 2).
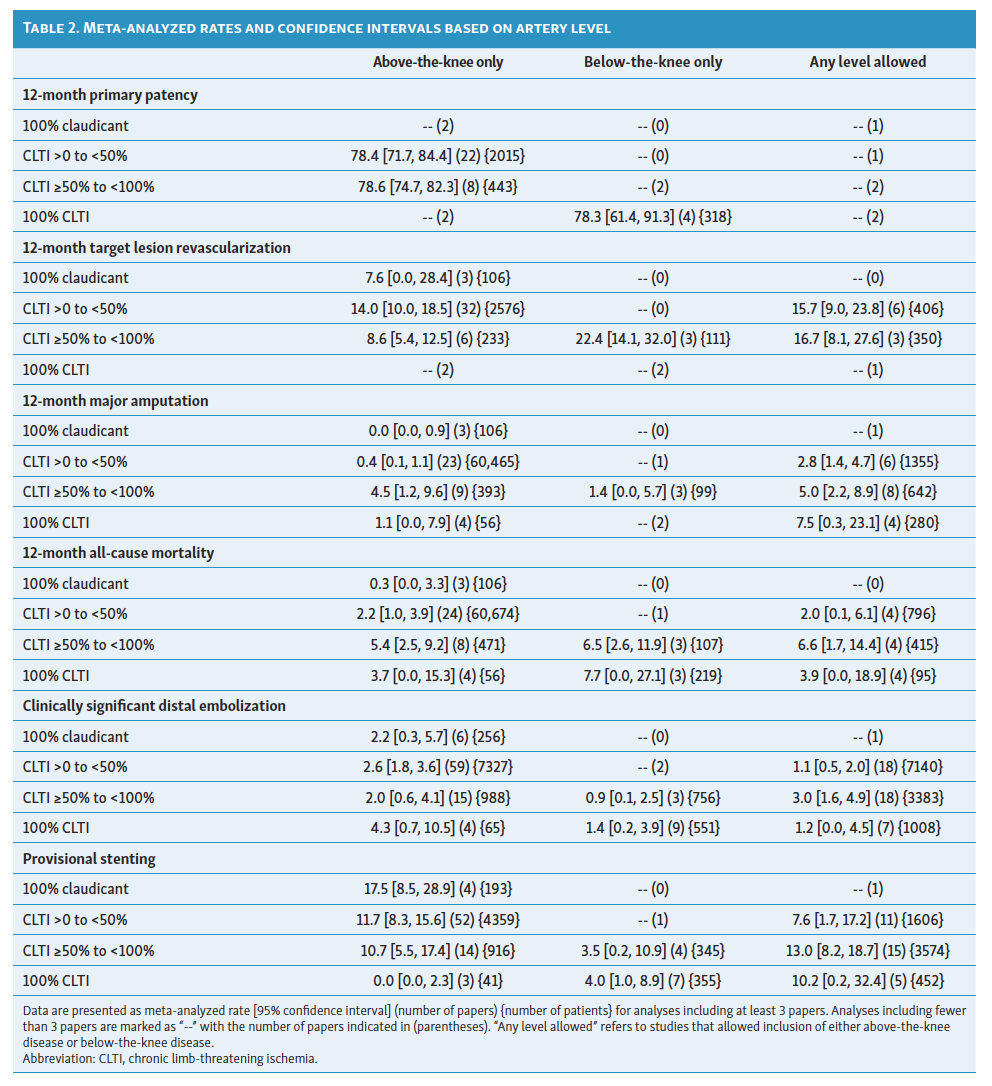
Results stratified by artery level are included in Table 2 for outcomes with a sufficient number of papers available for sub-stratification analysis. Of note, only 3 to 4 studies were available for the evaluation of 12-month clinical results among those that exclusively evaluated BTK disease. Patency was similar in papers that evaluated CLTI patients with BTK disease (78.3%) compared to papers including mixed cohorts with ATK disease (78.4% for the CLTI >0 to <50% group and 78.6% for the CLTI ≥50% to <100% group). In the CLTI ≥50% to <100% group, TLR was 8.6% for ATK disease cohorts (6 papers with 233 patients) vs 22.4% for BTK disease cohorts (3 papers with 111 patients). Among the 100% CLTI cohort, mortality was higher in papers evaluating BTK disease (7.7% across 3 papers) vs papers evaluating ATK disease (3.7% across 4 papers). The rates of clinically significant distal embolization were similarly low across most subsets evaluated. Provisional stenting rates were lower in BTK disease than in ATK disease, consistent with the previously published overall analysis.17
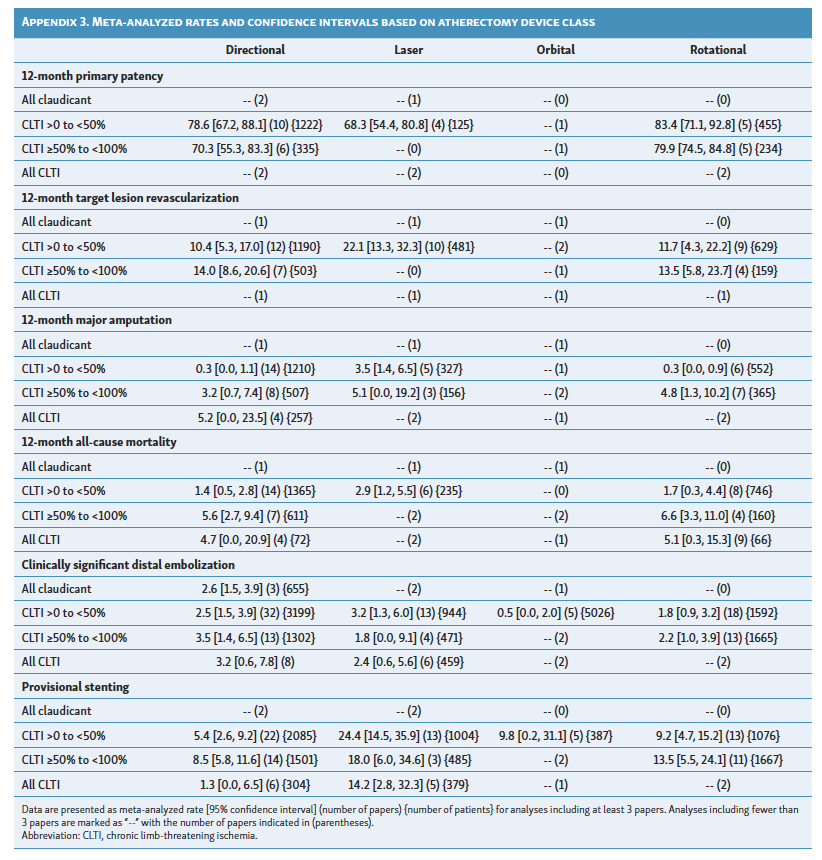
Sub-stratification of outcomes based on class of atherectomy device is shown in Appendix 3. Only directional and rotational atherectomy had sufficient data for meta-analysis across most clinical outcomes; the pattern of results was consistent with the overall analysis. Results based on device class in the full meta-analysis have been previously published.17
Discussion
Atherectomy can be used to prepare the vessel for definitive treatment and has a large volume of published data spanning over 35 years.17 However, more data are needed to understand the safety and effectiveness of atherectomy based on disease severity.
This systematic review and meta-analysis evaluated the quality and outcomes of atherectomy studies in patients with claudication, CLTI, or in mixed cohorts based on CLTI prevalence. While heterogeneity was observed across studies in this intentionally broad review, study cohorts with increased prevalence of CLTI patients exhibited expectedly longer lesions compared to 100% claudicant cohorts as well as a greater proportion of patients with total occlusions and TASC C/D lesions. Of note, the evaluation of CLTI across the published studies was not restricted to BTK disease; 20% of papers that evaluated CLTI enrolled only ATK lesions.
Despite exhibiting higher lesion complexity, increasing CLTI prevalence did not dramatically worsen 12-month effectiveness, with overlapping confidence intervals observed for both the TLR rates and the primary patency rates across the 4 cohorts evaluated. Patency was also similar regardless of artery level, with nearly identical rates in CLTI BTK disease cohorts compared to ATK cohorts regardless of the prevalence of CLTI. In fact, patency rates trended higher in the CLTI cohort (82.8%) compared to the claudicant cohort (68.4%), although this trend must be interpreted with caution given the lack of significance testing and a small sample size in the claudicant cohort. In the prospective, 47-center DEFINITIVE LE study, the 12-month rates of primary patency (defined as peak systolic velocity ratio ≤2.4) following directional atherectomy were 78.0% (95% CI 74.0-80.6) in the claudicant cohort vs 71.0% (95% CI 64.6-76.5) in the CLTI cohort in the overall analysis.26 In the infrapopliteal subset of DEFINITIVE LE, 1-year primary patency was 84% in claudicants and 78% in CLTI patients (P = .11).28 The meta-analyzed 12-month TLR rates in the current analysis were also similar across the CLTI subgroups, at 14.3% among 38 atherectomy studies with >0 to <50% prevalence of CLTI patients compared to 13.9% among 12 studies with ≥50% to <100% CLTI patients, suggesting a minimal impact of CLTI presence on TLR. However, the presence of BTK disease (vs ATK disease) appeared to have a greater impact on effectiveness than CLTI prevalence alone: among papers including ≥50% to <100% CLTI patients, TLR was 8.6% for ATK disease (6 papers) and 22.4% for BTK disease (3 papers). In comparison to angioplasty, a 52-study meta-analysis of uncoated balloon angioplasty without atherectomy for infrapopliteal disease reported 1-year repeat revascularization rates of 16% in cohorts consisting of <80% RCC 5/6 patients vs 21.3% in cohorts with ≥80% RCC 5/6 patients, with a similar pattern reported for primary patency (66.7% vs 56.3%, respectively).29 Effectiveness outcomes in the current atherectomy meta-analysis therefore appear better than meta-analyzed outcomes of standard balloon angioplasty, with CLTI prevalence exhibiting less of a detrimental effect on outcomes than artery level.
Pure CLTI cohorts were evaluated in relatively few studies. One-year primary patency was 82.8% across 8 studies while the 1-year TLR rate was 13.4% across 5 studies. In the LIBERTY 360 study of patients with CLTI treated with uncoated balloon angioplasty, orbital atherectomy, and/or stents, the 12-month cumulative incidence of target vessel revascularization was 27.9%.30 A meta-analysis of 44 studies (8602 CLTI patients) reported worse 1-year primary patency rates than the current atherectomy meta-analysis in infrapopliteal lesions (50% for bare metal stents, 73% for drug-eluting stents, and 66% for uncoated balloon angioplasty), and similar patency rates for uncoated balloon angioplasty in superficial femoral artery lesions (86%).31 The 1-year TLR rate of 13.4% in the current analysis also compares favorably to patients treated with paclitaxel DCBs without atherectomy in a large, global registry (14.1% in RCC 4-5 patients).32 However, comparisons are difficult since the current analysis included both uncoated balloon and DCB adjunctive therapies. For example, of the 5 studies reporting 1-year TLR in pure CLTI cohorts, adjunctive therapies consisted of DCB, plain old balloon angioplasty, or specialty balloons.33-36 Nonetheless, these results are encouraging and suggest that vessel preparation with atherectomy provides similar or better effectiveness in CLTI populations compared to other endovascular technologies.
Use of atherectomy in patients with claudication has been debated, with several reports suggesting an increased risk of reintervention in endovascular procedures using atherectomy (vs non-atherectomy percutaneous transluminal angioplasty [PTA]) for femoropopliteal claudication.37-39 However, outcomes are likely impacted by many factors. The current analysis identified only 3 papers reporting 12-month TLR in 100% claudicant cohorts, all including a high proportion of calcified lesions. These papers evaluated directional atherectomy plus DCB (0.0% TLR in 19 patients, all with severe calcification),24 orbital atherectomy plus uncoated balloon angioplasty (8.2% TLR in 25 patients, approximately half with calcification),27 or laser atherectomy plus uncoated balloon angioplasty (23.1% TLR in 65 patients, 61.5% with moderate/severe calcification).25 Combining atherectomy with adjunctive DCB therapy has also been shown to be more effective than atherectomy followed by uncoated balloon angioplasty in treating claudication.24,25,27 Thus, outcomes in patients with claudication are difficult to interpret in the present meta-analysis, with heterogeneity based on the extent of lesion calcification, class of atherectomy device used, and type of adjunctive therapy.
Safety outcomes in the current analysis were favorable compared to previously published rates for other endovascular procedures. Twelve-month rates of major amputation and mortality were expectedly higher in the 100% CLTI vs the 100% claudicant cohorts, as well as in mixed cohorts with an increased prevalence of CLTI. However, outcomes in this atherectomy analysis compare favorably to the 12-month major amputation and mortality rates of other endovascular procedures and bypass surgery. Meta-analyzed 1-year major amputation rates for atherectomy were 4.1% in the 20 studies including ≥50 to <100% CLTI patients and 5.8% in the 10 studies including 100% CLTI cohorts. Stratified by artery level, the 1-year major amputation rate was only 1.1% in CLTI patients with ATK disease, albeit in only 4 papers with 56 patients in total. In comparison, 1-year major amputation in CLTI patients was 10.4% in the LIBERTY 360 CLTI analysis (including 76% with BTK disease) after treatment with balloon angioplasty, atherectomy, or stents.30 One-year major amputation rates were 5.3% for PTA, 5.1% for stenting, and 7.1% for bypass surgery in a Medicare analysis of CLTI patients40 and 5% in a meta-analysis of 22 DCB studies.41 Similarly, meta-analyzed 1-year mortality rates for atherectomy in the current study were 6.1% in 15 studies including ≥50 to <100% CLTI patients and 5.0% in 11 studies including 100% CLTI cohorts. Mortality rates were higher in CLTI patients with BTK disease (7.7%) vs CLTI patients with ATK disease (3.7%). In comparison to the literature, 1-year mortality has been reported at 22% for untreated CLTI.1 In the BEST-CLI study,42 1-year mortality was approximately 14% in the cohort 2 endovascular group compared to approximately 18% in the surgery group, which is consistent with a 13.3% mortality rate in the LIBERTY 360 analysis of all endovascular procedures.30 In a 2020 meta-analysis of DCB for CLTI, 12-month mortality was 9% across 9 studies,41 which was corroborated by an 8.8% rate in a 2022 meta-analysis of DCB for infrapopliteal disease, including 84.5% CLTI patients and 15.5% claudicants.43 Finally, 1-year mortality was reported at 23.7% for PTA, 21.9% for stenting, and 21.8% for bypass surgery in a Medicare analysis of CLTI patients.40 Thus, despite expectedly higher mortality and amputation rates in studies evaluating more CLTI patients, outcomes following atherectomy are acceptable, with similar or better rates compared to other endovascular techniques.
Aligned with the previously published overall analysis of this dataset,17 the rate of provisional stenting was low compared to studies of uncoated balloon angioplasty and DCBs,29,44 possibly due to the ability of atherectomy to reduce plaque burden and prepare the vessel for angioplasty. As noted previously,17 provisional stenting was unsurprisingly lower for BTK disease than for ATK disease, with a lesser impact of CLTI prevalence.
Limitations
This intentionally broad meta-analysis evaluated atherectomy as a vessel preparation tool across a variety of scenarios, including study design, device types, patient and lesion characteristics, and type of adjunctive therapy used. As such, while providing valuable real-world data, heterogeneity was observed across studies. Most of the publications reviewed were observational and only 8.3% were randomized, impacting the interpretation of the results. A small number of studies in some analyses (and associated high variance), as well as variations in lesion characteristics and devices used, also limit interpretability. Variations in definitions, particularly primary patency, may have also influenced the results. Information on cardiovascular risk factors and comorbidities was not collected. Finally, due to the smaller number of studies reporting results beyond 1-year, longer-term follow-up is not available in this analysis.
Conclusions
Vessel preparation with atherectomy plays a primary role in any endovascular procedure with the goals of maximizing lumen gain, avoiding stent placement in high-risk territories, and delivering antirestenotic therapy. This is an important endeavor for both CLTI and claudicant patients. This meta-analysis demonstrates that atherectomy is associated with good TLR and primary patency rates and little evidence of complications. While effectiveness outcomes were similar regardless of the prevalence of CLTI, amputation and mortality were predictably worsened by increasing CLTI prevalence and BTK disease, though still lower than non-atherectomy literature comparators. As importantly, this meta-analysis demonstrates the large body of evidence supporting the role of adjunctive atherectomy during endovascular treatment of appropriately selected patients with claudication or CLTI. The decision to use atherectomy should be guided by evidence-based consideration of patient and lesion characteristics, and further studies are needed to better define its role in the treatment of peripheral vascular disease.
Acknowledgements
Biostatistical analysis was provided by Nick Salkowski, PhD, and Jeremiah Menk, MS, of Medtronic (Minneapolis, MN). Data extraction and verification were provided by Sangeeta Yendrembam, PhD, and Melissa Gaeta, MS, of Medtronic.
Click here to read a commentary on this article by Drs Dipankar Mukherjee and Richard Neville.
Affiliations and Disclosures
Jeffrey G. Carr, MD*, is from Interventional Cardiology, CHRISTUS Health – Heart and Vascular Institute, Tyler, Texas; Ralf Langhoff, MD*is from the Department of Angiology and Vascular Medicine, Sankt Gertrauden Hospital, Humboldt University Berlin, Germany; Brian G. DeRubertis, MD, is from the Division of Vascular and Endovascular Surgery, NewYork-Presbyterian Weill Cornell Medicine, New York, New York; Kristin L. Hood, PhD, is from Clinical Research and Medical Science, Medtronic, Plymouth, Minnesota; Prakash Krishnan, MD, is from Endovascular Services, The Mount Sinai Hospital, New York, New York; Vikram Puttaswamy, MD, is from Vascular and Renal Transplant Surgery, Royal North Shore Hospital, Sydney, Australia; Thomas Zerr, MD, PhD, is from University Heart Center Freiburg – Bad Krozingen, Bad Krozingen, Germany; and Eric A. Secemsky, MD, MSc*, is from Vascular Intervention, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts.
*Contributed equally
Presented at the Amputation Prevention Symposium (AMP) on August 14, 2025 by Eric Secemsky, MD and at AMP Europe on October 13, 2025 by Ralf Langhoff, MD.
One or more of the authors have disclosed potential financial or nonfinancial conflicts of interest regarding the content herein, as reported below. This work was funded and supported by Medtronic.
Dr Carr reports consultancy payments from Abbott, Becton Dickinson, Boston Scientific, Cordis, Medtronic, and Philips; speaking payments from Abbott, Becton Dickinson, Boston Scientific, Medtronic, and Philips; and stock in Avive, CDS, Fastwave Medical, Immertec, Sana, Vantis Vascular, and 2MG. Dr Langhoff reports consultancy payments from Biotronik, Contego Medical, Kardionet, and Medtronic. Dr DeRubertis reports consultancy payments from Abbott, Boston Scientific, Becton Dickinson, Cagent Vascular, and Medtronic. Dr Hood is a full-time employee and stockholder of Medtronic. Dr Krishnan reports consultancy payments from Abbott and Medtronic. Dr Puttaswamy reports consultancy payments from Medtronic, Boston Scientific, Gore & Associates, Artivion, and Philips. Dr Zeller reports consultancy payments from Abbott, Advanced NanoTherapies, Bayer, Boston Scientific, Gore & Associates, Medtronic, Philips-IntactVascular, Shockwave, Veryan, VentureMed, and Vesper Medical; speaking honoraria from Abbott, BIBA Medical, Biotronik, Boston Scientific, Cook Medical, Efemoral, Gore & Associates, Medtronic, Philips-Spectranetics, Shockwave, and Veryan; and research grants from Abbott, Bard Peripheral Vascular, B. Braun, Biotronik, Boston Scientific, Cook Medical, Gore & Associates, Intact Vascular, Med Alliance, Medtronic, Pluristem, Philips, PQ Bypass, Terumo, TriReme, Shockwave, Veryan, and University of Jena. Dr Secemsky reports consultancy or speaking payments from Abbott, Becton Dickinson, Bristol Myers Squibb, Boston Scientific, Cagent, Conavi, Cook, Cordis, Endovascular Engineering, Gore, InfraRedx, Medtronic, Philips, Rampart, RapidAI, Shockwave, Terumo, Thrombolex, VentureMed, and Zoll; and institutional research grants from Abbott, Becton Dickinson, Boston Scientific, Cook, Medtronic, and Philips.
Manuscript accepted March 17, 2026.
Address for correspondence: Eric A. Secemsky, MD, Beth Israel Deaconess Medical Center, 375 Longwood Avenue, Suite 440, Boston, MA 02215. Email: esecemsk@bidmc.harvard.edu
Appendices
Appendix 1. Papers included in the meta-analysis
Individual counts sum to more than 180 due to multiple subgroups in 6 papers.
All Claudicant Cohort (N = 13 papers)
1. Babaev A, Zavlunova S, Attubato MJ, Martinsen BJ, Mintz GS, Maehara A. Orbital atherectomy plaque modification assessment of the femoropopliteal artery via intravascular ultrasound (TRUTH Study). Vasc Endovascular Surg. 2015;49(7):188-194. doi:10.1177/1538574415607361
2. Babaev A, Halista M, Bakirova Z, Avtushka Matsumura M, Maehara A. Directional versus orbital atherectomy of femoropopliteal artery lesions: angiographic and intravascular ultrasound outcomes. Catheter Cardiovasc Interv. 2022;100(4):687-695. doi:10.1002/ccd.30339
3. Dave RM, Patlola R, Kollmeyer K, et al. Excimer laser recanalization of femoropopliteal lesions and 1-year patency: results of the CELLO registry. J Endovasc Ther. 2009;16(6):665-675. doi:10.1583/09-2781.1
4. Dregely I, Koppara T, Nekolla SG, et al. Observations with simultaneous 18F-FDG PET and MR imaging in peripheral artery disease. JACC Cardiovasc Imaging. 2017;10(6):709-711. doi:10.1016/j.jcmg.2016.06.005
5. Korogi Y, Hirai T, Sakamot Y, et al. Intravascular ultrasound imaging of peripheral arteries as an adjunct to atherectomy: preliminary experience. Br J Radiol.1995;68(806):110-115. doi:10.1259/0007-1285-68-806-110
6. Maehara A, Mintz GS, Shimshak TM, et al. Intravascular ultrasound evaluation of JETSTREAM atherectomy removal of superficial calcium in peripheral arteries. EuroIntervention. 2015;11(1):96-103. doi:10.4244/EIJV11I1A17
7. McKinsey JF, Zeller T, Rocha-Singh KJ, Jaff MR, Garcia LA, DEFINITIVE LE Investigators. Lower extremity revascularization using directional atherectomy: 12-month prospective results of the DEFINITIVE LE study. JACC Cardiovasc Interv. 2014;7(8):923-933. doi:10.1016/j.jcin.2014.05.006
8. Mukherjee D, Contos B, Emery E, Collins DT, Black JH, 3rd. High reintervention and amputation rates after outpatient atherectomy for claudication. Vasc Endovascular Surg. 2018;52(6):427-433. doi:10.1177/1538574418772459
9. Tarricone A, Ali Z, Rajamanickam A, et al. Histopathological evidence of adventitial or medial injury is a strong predictor of restenosis during directional atherectomy for peripheral artery disease. J Endovasc Ther. 2015;22(5):712-715. doi:10.1177/1526602815597683
10. Vroegindeweij D, Tielbeek AV, Buth J, Schol FP, Hop WC, Landman GH. Directional atherectomy versus balloon angioplasty in segmental femoropopliteal artery disease: two-year follow-up with color-flow duplex scanning. J Vasc Surg. 1995;21(2):255-269. doi: 10.1016/s0741-5214(95)70267-9
11. Wang H, Wu S, Pan D, et al. Real-world performance of excimer laser ablation combined with drug-coated balloon versus drug-coated balloon for the treatment of femoropopliteal in-stent restenosis disease. J Endovasc Ther. 2026;33(2):863-873. doi:10.1177/15266028241288778
12. Wilms G, Pauwels P, Peene P, et al. Percutaneous transluminal atherectomy: preliminary results. Cardiovasc Intervent Radiol. 1990;13(1):18-21. doi:10.1007/BF02576932
13. Zeller T, Langhoff R, Rocha-Singh KJ, et al; DEFINITIVE AR Investigators. Directional atherectomy followed by a paclitaxel-coated balloon to inhibit restenosis and maintain vessel patency: twelve-month results of the DEFINITIVE AR study. Circ Cardiovasc Interv. 2017;10(9):e004848. doi:10.1161/CIRCINTERVENTIONS.116.004848
CLTI >0 to <50% Cohort (N = 97 papers)
1. Avranas K, Pitoulias AG, Taneva GT, Beropoulis E, Donas KP. Sex-specific analysis of mid-term outcomes of atherectomy-assisted endovascular treatment in severe peripheral arterial disease. J Clin Med. 2024;13(11):3235. doi:10.3390/jcm13113235
2. Babaev A, Gokhale R, Zavlunova S, Attubato M. Treatment of angio-seal-related femoral artery occlusion using directional atherectomy-primary results and midterm follow-up. Vasc Endovascular Surg. 2016;50(8):541-546. doi:10.1177/1538574416679520
3. Baumgartner et al. Color-coded duplex sonography for evaluation of femoro-popliteal restenosis after percutaneous catheter atherectomy and subsequent transluminal balloon angioplasty. J Vasc Investigation. 1996;2:125-130.
4. Belli AM, Cumberland DC. Percutaneous atherectomy--early experience in Sheffield. Clin Radiol.1989;40(2):122-126. doi:10.1016/s0009-9260(89)80067-4
5. Böhme T, Romano L, Macharzina R, et al. Outcomes of directional atherectomy for common femoral artery disease. EuroIntervention. 2021;17(3):260-266. doi:10.4244/EIJ-D-19-00693
6. Böhme T, Noory E, Beschorner U, et al. Photoablative atherectomy followed by a paclitaxel-coated balloon to inhibit restenosis in instent femoro-popliteal obstructions (PHOTOPAC). Vasa. 2021;50(5):387-393. doi:10.1024/0301-1526/a000959
7. Burckenmeyer F, Aschenbach R, Diamantis I, Teichgräber U. Excimer laser atherectomy in complex peripheral artery disease: a prospective European registry. J Cardiovasc Surg (Torino). 2021;62(2):153-161. doi:10.23736/S0021-9509.21.11569-1
8. Cai Z, Guo L, Qi L, et al. Midterm outcome of directional atherectomy combined with drug-coated balloon angioplasty versus drug-coated balloon angioplasty alone for femoropopliteal arteriosclerosis obliterans. Ann Vasc Surg. 2020;64:181-187. doi:10.1016/j.avsg.2019.06.014
9. Cantu D, Jawaid O, Kokkinidis D, et al. Outcomes of drug-coated balloon angioplasty vs. conventional balloon angioplasty for endovascular treatment of common femoral artery atherosclerotic disease. Cardiovasc Revasc Med. 2020;21(7):867-874. doi:10.1016/j.carrev.2019.11.008
10. Carr J, Bowman J, Watts M, Ouriel K, Dave R. United States Investigational Device Exemption study of the Revolution Peripheral Atherectomy System. J Vasc Surg. 2022;75(3):976-986.e4. doi:10.1016/j.jvs.2021.08.107
11. Cha J, Lee J, Ko Y, et al. Clinical outcomes of atherectomy plus drug-coated balloon versus drug-coated balloon alone in the treatment of femoropopliteal artery disease. Korean Circ J. 2022;52(2):123-133. doi:10.4070/kcj.2021.0246
12. Cioppa A, Stabile E, Popusoi G, et al. Combined treatment of heavy calcified femoro-popliteal lesions using directional atherectomy and a paclitaxel coated balloon: one-year single centre clinical results. Cardiovasc Revasc Med. 2012;13(4):219-223. doi:10.1016/j.carrev.2012.04.007
13. Czihal M, Findik Z, Bernau C, et al. embolic protection in complex femoropopliteal interventions: safety, efficacy and predictors of filter macroembolization. Cardiovasc Intervent Radiol. 2021;44(5):700-708. doi:10.1007/s00270-020-02717-w
14. Das T, Mustapha J, Indes J, et al. Technique optimization of orbital atherectomy in calcified peripheral lesions of the lower extremities: the CONFIRM series, a prospective multicenter registry. Catheter Cardiovasc Interv. 2014;83(1):115-122. doi:10.1002/ccd.25046
15. Das TS, Shammas NW, Yoho JA, et al. Solid state, pulsed-wave 355 nm UV laser atherectomy debulking in the treatment of infrainguinal peripheral arterial disease: The Pathfinder Registry. Catheter Cardiovasc Interv. 2024;103(6):949-962. doi:10.1002/ccd.31023
16. Davis T, Ramaiah V, Niazi K, Gissler HM, Crabtree T. Safety and effectiveness of the Phoenix Atherectomy System in lower extremity arteries: early and midterm outcomes from the prospective multicenter EASE study. Vascular. 2017;25(8):563-575. doi:10.1177/1708538117712383
17. Dippel EJ, Makam P, Kovach R et al; EXCITE ISR Investigators. Randomized controlled study of excimer laser atherectomy for treatment of femoropopliteal in-stent restenosis: initial results from the EXCITE ISR trial (EXCImer Laser Randomized Controlled Study for Treatment of FemoropopliTEal In-Stent Restenosis). JACC Cardiovasc Interv. 2015;8(1 Pt A):92-101. doi:10.1016/j.jcin.2014.09.009
18. Dong Z, Guo L, Tong Z, et al. A retrospective comparative study of mid-term outcomes of atherectomy, drug-coating balloon angioplasty, and plain old balloon angioplasty for isolated atherosclerotic popliteal artery lesions. J Clin Hypertens (Greenwich). 2024;26(11):1264-1273. doi:10.1111/jch.14908
19. Dorros G, Iyer S, Lewin R, Zaitoun R, Mathiak L, Olson K. Angiographic follow-up and clinical outcome of 126 patients after percutaneous directional atherectomy (Simpson AtheroCath) for occlusive peripheral vascular disease. Cathet Cardiovasc Diagn. 1991;22(2):79-84. doi:10.1002/ccd.1810220202
20. Ducasse E, Sapoval M, Brunet J, et al. Outcomes and comparative analysis of the initial results of standard balloon angioplasty versus drug-coated balloons alone versus in association with laser-excimer atherectomy in the treatment of femoropopliteal artery in-stent restenosis (INTACT). J Endovasc Ther. 2026:33(1):244-258. doi:10.1177/15266028241248333
21. Foley RT, Cotter RP, Kokkinidis DG, Nguyen DD, Waldo SW, Armstrong EJ. Mid-term outcomes of orbital atherectomy combined with drug-coated balloon angioplasty for treatment of femoropopliteal disease. Catheter Cardiovasc Interv. 2017;89(6):1078-1085. doi:10.1002/ccd.26984
22. Giannopoulos S, Kokkinidis DG, Jawaid O, et al. Turbo-power laser atherectomy combined with drug-coated balloon angioplasty is associated with improved one-year outcomes for the treatment of Tosaka II and III femoropopliteal in-stent restenosis. Cardiovasc Revasc Med. 2020;21(6):771-778. doi:10.1016/j.carrev.2019.10.006
23. Gonschior P, Höfling B, Mack B, et al. Results of directional peripheral atherectomy with reference to histology, histochemistry, and ultrastructure. Angiology. 1993;44(6):454-463. doi:10.1177/000331979304400605
24. Graor RA, Whitlow PL. Transluminal atherectomy for occlusive peripheral vascular disease. J Am Coll Cardiol. 1990;15(7):1551-1558. doi:10.1016/0735-1097(90)92825-m
25. Gray WA, Garcia LA, Amin A, Shammas NW, et al; JET Registry Investigators. Jetstream atherectomy system treatment of femoropopliteal arteries: results of the post-market JET Registry. Cardiovasc Revasc Med. 2018;19(5 Pt A):506-511. doi:10.1016/j.carrev.2017.12.015
26. Gumus F, Arslanturk O. Usage of rotational atherectomy and drug-coated balloon angioplasty for isolated popliteal artery lesions: two-year results of a retrospective study. Acta Chir Belg. 2024;124(5):365-371. doi:10.1080/00015458.2024.2313266
27. Guo J, Guo L, Tong Z, Gao X, Wang Z, Gu Y. Directional atherectomy is associated with better long-term efficiency compared with angioplasty for common femoral artery occlusive disease in rutherford 2-4 patients. Ann Vasc Surg. 2018;51:65-71. doi:10.1016/j.avsg.2017.12.004
28. Henry M, Amor M, Ethevenot G, Henry I, Allaoui M. Percutaneous peripheral atherectomy using the rotablator: a single-center experience. J Endovasc Surg.1995;2(1):51-66. doi:10.1583/1074-6218(1995)002<0051:PPAUTR>2.0.CO;2
29. Hinohara T, Selmon MR, Robertson GC, Braden L, Simpson JS. Directional atherectomy. New approaches for treatment of obstructive coronary and peripheral vascular disease. Circulation. 1990;81(3 Suppl):IV79-91.
30. Höfling B, Pölnitz AV, Backa D, et al. Percutaneous removal of atheromatous plaques in peripheral arteries. Lancet. 1988;1(8582):384-386. doi:10.1016/s0140-6736(88)91183-x
31. Imran HM, Hyder ON, Soukas PA. Efficacy and safety of adjunctive drug-coated balloon therapy in endovascular treatment of common femoral artery disease. Cardiovasc Revasc Med. 2019;20(3):210-214. doi:10.1016/j.carrev.2018.06.018
32. Israni N, Lee J, Bai H, et al. Women are not at higher risk for reintervention or major amputation after lower extremity atherectomy for peripheral artery disease. Ann Vasc Surg. 2023;95:95-107. doi:10.1016/j.avsg.2023.04.001
33. Jahnke T, Link J, Müller-Hülsbeck S, Grimm J, Heller M, Brossman J. Treatment of infrapopliteal occlusive disease by high-speed rotational atherectomy: initial and mid-term results. J Vasc Interv Radiol. 2001;12(2):221-226. doi:10.1016/s1051-0443(07)61829-6
34. Janas A, Buszman PP, Milewski KP, et al. Long-term outcomes after percutaneous lower extremity arterial interventions with atherectomy vs. balloon angioplasty - propensity score-matched registry. Circ J. 2017;81(3):376-382. doi:10.1253/circj.CJ-16-0856
35. Janas A, Milewski K, Buszman P, et al. Comparison of long-term outcomes after directional versus rotational atherectomy in peripheral artery disease. Postepy Kardiol Interwencyjnej. 2020;16(1):76-81. doi:10.5114/aic.2020.93914
36. Kavala AA, Kuserli Y, Turkyilmaz G, Yesiltas MA, Turkyilmaz S. Comparison of drug-coated balloon angioplasty alone and directional atherectomy combined with drug-coated balloon angioplasty in patients with lower extremity peripheral arterial disease with claudication. Ann Vasc Surg. 2023;90:162-171. doi:10.1016/j.avsg.2022.10.007
37. Kim HJ, Hwang D, Yun W, Huh S, Kim H. Effectiveness of atherectomy and drug-coated balloon angioplasty in femoropopliteal disease: a comprehensive outcome study. Vasc Specialist Int. 2024;40:34. doi:10.5758/vsi.240071
38. Kokkinidis DG, Hossain P, Jawaid O, et al. Laser atherectomy combined with drug-coated balloon angioplasty is associated with improved 1-year outcomes for treatment of femoropopliteal in-stent restenosis. J Endovasc Ther. 2018;25(1):81-88. doi:10.1177/1526602817745668
39. Kokkinidis DG, Jawaid O, Cantu D, et al. Two-year outcomes of orbital atherectomy combined with drug-coated balloon angioplasty for treatment of heavily calcified femoropopliteal lesions. J Endovasc Ther. 2020;27(3):492-501. doi:10.1177/1526602820915244
40. Kolvenbach R, Strosche H. Long term results after rotation angioplasty and catheter atherectomy. A retrospective analysis. J Cardiovasc Surg (Torino).1998;39(1):15-18.
41. Korosoglou G, Feld J, Langhoff R, et al; RECCORD Investigators. Safety and effectiveness of debulking for the treatment of infrainguinal peripheral artery disease. Data from the Recording Courses of Vascular Diseases registry in 2910 patients. Angiology. 2025:76(10):981-990. doi:10.1177/00033197241263381
42. Krawisz AK, Raja A, Jones WS, et al. Long-term outcomes of peripheral atherectomy for femoropopliteal endovascular interventions. EuroIntervention. 2023;18(16):e1378-e1387. doi:10.4244/EIJ-D-22-00609
43. Kronlage M, Erbel C, Lichtenberg M, et al. Safety and effectiveness of Phoenix atherectomy for endovascular treatment in calcified common femoral artery lesions. Vasa. 2021;50(5):378-386. doi:10.1024/0301-1526/a000960
44. Kronlage M, Bertele M, Linden F, Frey N, Erbel C. Stand-Alone rotational atherectomy versus combination with drug-coated balloon angioplasty for the endovascular treatment of heavily-calcified femoropopliteal and popliteal lesions. J Endovasc Ther. 2025:32(5):1699-1706. doi:10.1177/15266028231219663
45. Laird JR Jr, Yeo KK, Rocha-Singh K, et al. Excimer laser with adjunctive balloon angioplasty and heparin-coated self-expanding stent grafts for the treatment of femoropopliteal artery in-stent restenosis: twelve-month results from the SALVAGE study. Catheter Cardiovasc Interv. 2012;80(5):852-859. doi:10.1002/ccd.23475
46. Lee Y, Ko Y, Ahn C, et al. Outcomes of adjunctive drug-coated versus uncoated balloon after atherectomy in femoropopliteal artery disease. Ann Vasc Surg. 2020;68:391-399. doi:10.1016/j.avsg.2020.04.032
47. Li, et al. Midterm outcome of directional atherectomy versus plain balloon angioplasty with adjunctive stenting for femoropopliteal artery lesions: s single-center experience. Vascular Investigation and Therapy. 2020;3:33.
48. Liu H, Gu Y, Yang S, He J, Zhang F. Excimer laser atherectomy combined with drug-coated balloon angioplasty for the treatment of chronic obstructive femoropopliteal arterial disease. Exp Ther Med. 2020;19(3):1887-1895. doi:10.3892/etm.2019.8362
49. Lodha A, Giannopoulos S, Sumar R, et al. Transradial endovascular intervention: results from the Radial accEss for nAvigation to Your CHosen Lesion for Peripheral Vascular Intervention (REACH PVI) study. Cardiovasc Revasc Med. 2022;36:115-120. doi:10.1016/j.carrev.2021.05.011
50. Lüdtke CW, Scheer F, Kamusella P, Wissgott, Andresen R. Transpopliteal balloon-assisted excimer-laser atherectomy for the treatment of chronic femoropopliteal occlusions: feasibility and initial results. Clin Med Insights Cardiol. 2015;8(Suppl 2):23-28. doi:10.4137/CMC.S15230
51. Ma Z, Feng T, Zheng D, Duman B. Application of TurboHawk plaque rotary cutting system in the treatment of lower extremity arteriosclerosis obliterans. Safety and efficacy. Ital J Vasc Endovasc Surg. 2022;29(1):20-27. doi:10.23736/S1824-4777.21.01525-4
52. Makam P. Use of orbital atherectomy treatment in a high-volume clinical practice modifies non-compliant plaque to deliver durable long-term results. J Invasive Cardiol. 2013;25(2):85-88.
53. Mehta M, Zhou Y, Paty PSK, et al. Percutaneous common femoral artery interventions using angioplasty, atherectomy, and stenting. J Vasc Surg. 2016;64(2):369-379. doi:10.1016/j.jvs.2016.03.418
54. Newman GE, Miner DG, Sussman SK, et al. Peripheral artery atherectomy: description of technique and report of initial results. Radiology. 1988;169(3):677-680. doi:10.1148/radiology.169.3.2973078
55. Noory E, Böhme T, Steinhauser Y, et al. Acute and mid-term results of atherectomy in femoropopliteal lesions. J Endovasc Ther. 2025;32(6):2137-21146. doi:10.1177/15266028241240898
56. Osborn JJ, Pfeiffer RB Jr, String ST. Directional atherectomy and balloon angioplasty for lower extremity arterial disease. Ann Vasc Surg. 1997;11(3):278-283. doi:10.1007/s100169900046
57. Ott I, Cassese S, Groha P, et al. Randomized comparison of paclitaxel-eluting balloon and stenting versus plain balloon plus stenting versus directional atherectomy for femoral artery disease (ISAR-STATH). Circulation. 2017;135(23):2218-2226. doi:10.1161/CIRCULATIONAHA.116.025329
58. Pan D, Guo J, Su Z, et al. Safety and efficacy of excimer laser atherectomy combined with a drug-coated balloon in de novo femoral popliteal artery disease: a retrospective study. Ann Vasc Surg. 2024;99:26-32. doi:10.1016/j.avsg.2023.09.072
59. Park Y, Heo S, Hyun D, et al. Usefulness of intraoperative ultrasonography during directional atherectomy using SilverHawk/TurboHawk system. Ann Surg Treat Res. 2017;92(1):42-46. doi:10.4174/astr.2017.92.1.42
60. Picazo F, Kwok RCH, Hockley JA, Garbowski MW, Samuelson SD, Jansen SJ. Directional atherectomy of the common femoral artery: complications and outcomes. Ann Vasc Surg. 2020;66:621-630. doi:10.1016/j.avsg.2020.01.094
61. Ramaiah V, Gammon R, Kiesz S, et al; TALON Registry. Midterm outcomes from the TALON Registry: treating peripherals with SilverHawk: outcomes collection. J Endovasc Ther. 2006;13(5):592-602. doi:10.1583/05-1780MR.1
62. Rastan A, Sixt S, Schwarzwälder U, et al. Initial experience with directed laser atherectomy using the CLiRpath photoablation atherectomy system and bias sheath in superficial femoral artery lesions. J Endovasc Ther. 2007;14(3):365-373. doi:10.1583/06-2046.1
63. Regine R, Catalano O, De Siero M, Di Costanzo G, Ragozzino A. Endovascular treatment of femoropopliteal stenoses/occlusions with a SilverHawk directional atherectomy device: immediate results and 12-month follow-up. Radiol Med. 2010;115(8):1208-1218. doi:10.1007/s11547-010-0570-8
64. Roberts D, Niazi K, Miller W, et al; DEFINITIVE Ca++ Investigators. Effective endovascular treatment of calcified femoropopliteal disease with directional atherectomy and distal embolic protection: final results of the DEFINITIVE Ca++ trial. Catheter Cardiovasc Interv. 2014;84(2):236-244. doi:10.1002/ccd.25384
65. Rocha-Singh KJ, Sachar R. DeRubertis BG, et al. Directional atherectomy before paclitaxel coated balloon angioplasty in complex femoropopliteal disease: the VIVA REALITY study. Catheter Cardiovasc Interv. 2021;98(3):549-558. doi:10.1002/ccd.29777
66. Rodoplu O, Oztas DM, Meric M, et al. Efficacy of rotational atherectomy followed by drug-coated balloon angioplasty for the treatment of femoropopliteal lesions-comparison with sole drug-coated balloon revascularization: two-year outcomes. Ann Vasc Surg. 2021;73:222-233. doi:10.1016/j.avsg.2020.10.051
67. Safian RD, Niazi K, Runyon JP, et al; OASIS Investigators. Orbital atherectomy for infrapopliteal disease: device concept and outcome data for the OASIS trial. Catheter Cardiovasc Interv. 2009;73(3):406-412. doi:10.1002/ccd.21898
68. Sanon O, Carnevale M, Indes J, Gao Q, Lipsitz E, Koleilat I. Incidence of procedure-related complications in patients treated with atherectomy in the femoropopliteal and tibial vessels in the Vascular Quality Initiative. J Endovasc Ther. 2023;30(5):693-702. doi: 10.1177/15266028221091900
69. Schwindt AG, Bennett JG Jr, Crowder WH, et al. Lower extremity revascularization using optical coherence tomography-guided directional atherectomy: final results of the EValuatIon of the PantheriS OptIcal COherence Tomography ImagiNg Atherectomy System for Use in the Peripheral Vasculature (VISION) Study. J Endovasc Ther. 2017;24(3):355-366. doi:10.1177/1526602817701720
70. Shammas NW, Coiner D, Shammas GA, Dippel EJ, Christensen , Jerin M. Percutaneous lower-extremity arterial interventions with primary balloon angioplasty versus Silverhawk atherectomy and adjunctive balloon angioplasty: randomized trial. J Vasc Interv Radiol. 2011;22(9):1223-1228. doi:10.1016/j.jvir.2011.05.013
71. Shammas NW, Shammas GA, Helou TJ, Voelliger CM, Mrad L, Jerin M. Safety and 1-year revascularization outcome of SilverHawk atherectomy in treating in-stent restenosis of femoropopliteal arteries: a retrospective review from a single center. Cardiovasc Revasc Med. 2012;13(4):224-227. doi:10.1016/j.carrev.2012.03.004
72. Shammas NW, Shammas GA, Hafez A, Kelly R, Reynolds E, Shammas AN. Safety and one-year revascularization outcome of excimer laser ablation therapy in treating in-stent restenosis of femoropopliteal arteries: a retrospective review from a single center. Cardiovasc Revasc Med. 2012;13(6):341-344. doi:10.1016/j.carrev.2012.08.012
73. Shammas NW, Shammas GA, Banerjee S, Popma JJ, Mohammad A, Jerin M. JetStream rotational and aspiration atherectomy in treating in-stent restenosis of the femoropopliteal arteries: results of the JETSTREAM-ISR feasibility study. J Endovasc Ther. 2016;23(2):339-346. doi:10.1177/1526602816634028
74. Shammas NW, Shammas GA, Arikat L, et al. Five-year freedom from target-lesion revascularization using excimer laser ablation therapy in the treatment of in-stent restenosis of femoropopliteal arteries. J Invasive Cardiol. 2017;29(6):207-208.
75. Shammas NW, Shammas GA, Jones-Miller S, et al. Long-term outcomes with Jetstream atherectomy with or without drug coated balloons in treating femoropopliteal arteries: a single center experience (JET-SCE). Cardiovasc Revasc Med. 2018;19(7 Pt A):771-777.
76. Shammas NW, Petruzzi N, Henao S, et al. JetStream atherectomy for the treatment of in-stent restenosis of the femoropopliteal segment: one-year results of the JET-ISR study. J Endovasc Ther. 2021;28(1):107-116. doi:10.1177/1526602820951916
77. Shammas NW, Torey JT, Shammas WJ, Jones-Miller S, Shammas GA. Intravascular ultrasound assessment and correlation with angiographic findings of arterial dissections following Auryon laser atherectomy and adjunctive balloon angioplasty: results of the iDissection Auryon laser study. J Endovasc Ther. 2022;29(1):23-31. doi:10.1177/15266028211028200
78. Shammas NW, Purushottam B, Shammas WJ, et al. Jetstream atherectomy followed by paclitaxel-coated balloons versus balloon angioplasty followed by paclitaxel-coated balloons: twelve-month exploratory results of the prospective randomized JET-RANGER study. Vasc Health Risk Manag. 2022;18:603-615. doi:10.2147/VHRM.S371177
79. Sharis EM, Shammas NW, Shammas GA, Jones-Miller S. WIRION EPS filter with Jetstream atherectomy of femoropopliteal arterial disease: a single center experience. Cardiovasc Revasc Med. 2020;21(1):96-99. doi:10.1016/j.carrev.2018.11.014
80. Simpson JB, Selmon MR, Robertson GC, et al. Transluminal atherectomy for occlusive peripheral vascular disease. Am J Cardiol. 1988;61(14):96G-101G. doi:10.1016/s0002-9149(88)80040-7
81. Sixt S, Carpio Cancino OG, Treszi A, et al. Drug-coated balloon angioplasty after directional atherectomy improves outcome in restenotic femoropopliteal arteries. J Vasc Surg. 2013;58(3):682-686. doi:10.1016/j.jvs.2013.02.019
82. Staniloae CS, Korzbathina R, Lane TA, et al. Study to determine the clinical significance of HEmolysis During Orbital AtheRectomy (CLEAR study). J Endovasc Ther. 2011;18(1):57-63. doi:10.1583/10-3179.1
83. Stavroulakis K, Schwindt A, Torsello G, et al. Directional atherectomy with antirestenotic therapy vs drug-coated balloon angioplasty alone for isolated popliteal artery lesions. J Endovasc Ther. 2017;24(2):181-188. doi:10.1177/1526602816683933
84. Stavroulakis K, Schwindt A, Torsello G, et al. Directional atherectomy with antirestenotic therapy vs drug-coated balloon angioplasty alone for common femoral artery atherosclerotic disease. J Endovasc Ther. 2018;25(1):92-99. doi:10.1177/1526602817748319
85. Stavroulakis K, Bisdas T, Torsello G, Argyriou A, Bollenberg L, Schwindt A. Optical coherence tomography guided directional atherectomy with antirestenotic therapy for femoropopliteal arterial disease. J Cardiovasc Surg (Torino). 2019;60(2):191-197. doi:10.23736/S0021-9509.19.10843-9
86. Taneva GT, Pitoulias AG, Avranas K, et al. Midterm outcomes of rotational atherectomy-assisted endovascular treatment of severe peripheral arterial disease. J Vasc Surg. 2024;79(4):887-892. doi:10.1016/j.jvs.2023.12.030
87. Torsello GB, Melo RGE, Zeller T, et al. Atherectomy followed by drug-coated balloon angioplasty versus surgery for symptomatic deep femoral artery arteriosclerotic disease. J Endovasc Ther. 2024;15266028241284443. doi:10.1177/15266028241284443
88. Trentmann J, Charalambous N, Djawanscher M, Schäfer J, Jahnke T. Safety and efficacy of directional atherectomy for the treatment of in-stent restenosis of the femoropopliteal artery. J Cardiovasc Surg (Torino). 2010;51(4):551-560.
89. Visonà A, Perissinotto C, Lusiani L, et al. Percutaneous excimer laser angioplasty of lower limb vessels: results of a prospective 24-month follow-up. Angiology. 1998;49(2):91-98. doi:10.1177/000331979804900201
90. Werner-Gibbings K, Dubenec S. Short-term outcomes of excisional atherectomy in lower limb arterial disease. ANZ J Surg. 2017;87(6):E1-E4. doi:10.1111/ans.12897
91. Wildenhain PM, Wholey MH, Jarmolowski CR, Hill KL. Infrainguinal directional atherectomy: long-term follow-up and comparison with percutaneous transluminal angioplasty. Cardiovasc Intervent Radiol. 1994;17(6):305-311. doi:10.1007/BF00203948
92. Wissgott C, Kamusella P, Andresen R. Treatment of femoropopliteal stenoses and occlusions with mechanical rotational catheters: comparison of results with the Rotarex and Pathway devices. J Cardiovasc Surg (Torino). 2012;53(2):177-186.
93. Yang L, Quan J, Dong J, et al. Comparison of mid-outcome among bare metal stent, atherectomy with or without drug-coated balloon angioplasty for femoropopliteal arterial occlusion. Sci Rep. 2024;14(1):63. doi:10.1038/s41598-023-50511-8
94. Yiğit G. Early outcomes of novel Temren atherectomy device combined with drug-coated balloon angioplasty for treatment of femoropopliteal lesions. Vascular. 2022;30(4):739-748. doi:10.1177/17085381211029819
95. Yongquan G, Lianrui G, Lixing Q, et al. Plaque excision in the management of lower-limb ischemia of atherosclerosis and in-stent restenosis with the SilverHawk atherectomy catheter. Int Angiol. 2013;32(4):362-367.
96. Yuan Z. Yang B, Wang J, An H, Xu H. TurboHawk plaque rotation system for treatment of arteriosclerosis occlusion in lower extremities: a pilot retrospective study. Medicine (Baltimore). 2021;100(5):e23976. doi:10.1097/MD.0000000000023976
97. Zeller T, Langhoff R, Rocha-Singh KJ, et al; DEFINITIVE AR Investigators. Directional atherectomy followed by a paclitaxel-coated balloon to inhibit restenosis and maintain vessel patency: twelve-month results of the DEFINITIVE AR study. Circ Cardiovasc Interv. 2017;10(9):e004848. doi:10.1161/CIRCINTERVENTIONS.116.004848
CLTI ≥50% to <100% Cohort (N = 51 papers)
1. The Collaborative Rotablator Atherectomy Group (CRAG). Peripheral atherectomy with the rotablator: a multicenter report. J Vasc Surg. 1994;19(3):509-515. doi:10.1016/s0741-5214(94)70079-6
2. Ali M, Noureldin M, Elokda A, Tawfik A. Comparative study between mechanical rotational atherectomy combined with drug-coated balloon versus drug-coated balloon alone for treatment of in-stent restenosis during peripheral endovascular interventions: a multicentric trial. J Vasc Dis. 2024;3(3):290-305. doi:10.3390/jvd3030023
3. Ansaarie I, Goldfaden RF, Hard J, et al. A retrospective cohort study to evaluate the efficacy, safety, and cost of MáLEI via transradial vs transfemoral peripheral revascularizations. Vascular Disease Management. 2021;18(10):E178-E183.
4. Ardita V, Ronchey S, Orrico M, et al. Jetstream atherectomy system for treatment of femoropopliteal artery disease: a single center experience and mid-term outcomes. Ann Vasc Surg. 2020;62:365-374. doi:10.1016/j.avsg.2019.04.052
5. Avranas K, Pitoulias AG, Taneva GT, Beropoulis E, Donas KP. Sex-specific analysis of mid-term outcomes of atherectomy-assisted endovascular treatment in severe peripheral arterial disease. J Clin Med. 2024;13(11):3235. doi:10.3390/jcm13113235
6. Cioppa A, Stabile E, Salemme L, et al. Combined use of directional atherectomy and drug-coated balloon for the endovascular treatment of common femoral artery disease: immediate and one-year outcomes. EuroIntervention. 2017;12(14):1789-1794. doi:10.4244/EIJ-D-15-00187
7. Dumantepe M. Retrograde popliteal access to percutaneous peripheral intervention for chronic total occlusion of superficial femoral arteries. Vasc Endovascular Surg. 2017;51(5):240-246. doi:10.1177/1538574417698902
8. Engin AY, Saydam O. Rotational atherectomy with adjunctive balloon angioplasty in calcified chronic total occlusions of superficial femoral artery. Vascular. 2021;29(5):682-692. doi:10.1177/1708538120970817
9. Feng Z, Yang S, Sang H, et al. One-year clinical outcome and risk factor analysis of directional atherectomy followed with drug-coated balloon for femoropopliteal artery disease. J Endovasc Ther. 2021;28(6):927-937. doi:10.1177/15266028211030527
10. Gandini R. Pratesi G, Merolla S, Scaggiante J, Chegai F. A single-center experience with phoenix atherectomy system in patients with moderate to heavily calcified femoropopliteal lesions. Cardiovasc Revasc Med. 2020;21(5):676-681. doi:10.1016/j.carrev.2019.08.019
11. Giannopoulos S, Secemsky EA, Mustapha JA, et al. Three-year outcomes of orbital atherectomy for the endovascular treatment of infrainguinal claudication or chronic limb-threatening ischemia. J Endovasc Ther. 2020;27(5):714-725. doi:10.1177/1526602820935611
12. Giusca S, Lichtenberg M, Schueler M, et al. Safety, effectiveness and mid-term follow-up in 136 consecutive patients with moderate to severely calcified lesions undergoing phoenix atherectomy. Heart Vessels. 2021;36(3):366-375. doi:10.1007/s00380-020-01695-w
13. Giusca S, Hagstptz S, Lichtenberg M, et al. Phoenix atherectomy for patients with peripheral artery disease. EuroIntervention. 2022;18(5):e432-e442. doi:10.4244/EIJ-D-21-01070
14. Grubnic S, Heenan SD, Buckenham TM, Belli AM. Evaluation of the pullback atherectomy catheter in the treatment of lower limb vascular disease. Cardiovasc Intervent Radiol. 1996;19(3):152-159.
15. Gu Y, Malas MB, Qi L, et al. A comparative study of percutaneous atherectomy for femoropopliteal arterial occlusive disease. Int Angiol. 2017;36(4):340-345. doi:10.23736/S0392-9590.17.03797-X
16. Guan S, Sun J, Jiareke T, Ge X. Evaluation of TurboHawk plaque rotation system in treatment of superficial femoral atherosclerosis. Med Sci Monit. 2018;24:9026-9031. doi:10.12659/MSM.912142
17. Hicks CW, Holscher CM, Wang P, et al. Use of atherectomy during index peripheral vascular interventions. JACC Cardiovasc Interv. 2021;14(16):678-688. doi:10.1016/j.jcin.2021.01.004
18. Hogan SE, Holland M, Burke J, et al. Retrospective review of directional atherectomy and drug-coated balloon use in a PAD safety-net population. J Invasive Cardiol. 2023;35(4):E205-E216. doi:10.25270/jic/22.00382
19. Ibáñez MA, Cenizo N, Río L. Clinical and haemodynamic evolution of lesions treated by means of atherectomy with SilverHawk in the femoropopliteal sector. Eur J Radiol. 2011;80(2):543-547. doi:10.1016/j.ejrad.2011.01.018
20. Ivan E, Martinsen B, Igyarto Z, Sublett T, Nachimuthu S. peripheral artery disease in vulnerable patient populations: outcomes of orbital atherectomy in Native Americans compared to non-Native Americans. A single-center experience in rural Oklahoma. Cardiovasc Revasc Med. 2021;22:71-77. doi:10.1016/j.carrev.2020.06.008
21. Janas A, Milewski K, Buszman P, et al. Comparison of long-term outcomes after directional versus rotational atherectomy in peripheral artery disease. Adv Intervent Cardiol. 2020;16(1):76-81. doi:10.5114/aic.2020.93914
22. Jiang X, Li X, Chen B, et al. Results of excimer laser ablation combined with drug-coated balloon for atherosclerotic obliterans of lower extremity and risk factors for loss of primary patency. Ann Vasc Surg. 2023;91:223-232. doi:10.1016/j.avsg.2022.11.026
23. Katsiki N, Geiss E, Giesen A, et al. Lesion localization and limb outcomes in elderly patients with and without type 2 diabetes mellitus who undergo atherectomy-assisted endovascular revascularization due to symptomatic peripheral artery disease. J Clin Med. 2024;13(21):6385. doi:10.3390/jcm13216385
24. Keeling WB, Shames ML, Stone PA, et al. Plaque excision with the Silverhawk catheter: early results in patients with claudication or critical limb ischemia. J Vasc Surg. 2007;45(1):25-31. doi:10.1016/j.jvs.2006.08.080
25. Khalili H, Jeon-Slaughter H, Armstrong EJ, et al. Atherectomy in below-the-knee endovascular interventions: one-year outcomes from the XLPAD registry. Catheter Cardiovasc Interv. 2019;93(3):488-493. doi:10.1002/ccd.27897
26. Kiesz RS, Wiernek SL, Wiernek BK, et al. Long-term results of plaque excision combined with aggressive pharmacotherapy in high-risk patients with advanced peripheral artery disease (SAVE a LEG registry). Catheter Cardiovasc Interv. 2013;82(3):E244-250. doi:10.1002/ccd.24756
27. Korabathina R, Mody KP, Yu J, Han SY, Patel R, Staniloae CS. Orbital atherectomy for symptomatic lower extremity disease. Catheter Cardiovasc Interv. 2010;76(3):326-332. doi:10.1002/ccd.22508
28. Kovaleski A. Trends in outcomes associated with the use of Auryon atherectomy system in a real-world setting. Cardiovasc Revasc Med. 2023;57:27-31. doi:10.1016/j.carrev.2023.06.020
29. Kumarasamy A, Gombert A, Krabbe J, Ruprecht O, Jacobs MJ, Krabbe H. Assessment of feasibility and patency of below the knee atherectomy using the 1.5 mm Phoenix catheter—a retrospective study. Medicina (Kaunas). 2022;58(11):1594. doi:10.3390/medicina58111594
30. Lin Y, Quan J, Dong J, Cong L, Yang L. The midterm outcomes of endovascular therapy for femoropopliteal lesions via drug-coated balloon, directional atherectomy and bare metal stent angioplasty. Rev Cardiovasc Med. 2024;25(9):331. doi:10.31083/j.rcm2509331
31. Loffroy R, Edriss N, Goyault G, et al. Percutaneous mechanical atherothrombectomy using the Rotarex® S device in peripheral artery in-stent restenosis or occlusion: a French retrospective multicenter study on 128 patients. Quant Imaging Med Surg. 2020;10(1):283-293. doi:10.21037/qims.2019.11.15
32. Mallios A, Blebea J, Buster B, Messiner R, Taubman K, Ma H. Laser atherectomy for the treatment of peripheral arterial disease. Ann Vasc Surg. 2017;44:269-276. doi:10.1016/j.avsg.2017.04.013
33. McKinsey JF. Goldstein L, Khan HU, et al. Novel treatment of patients with lower extremity ischemia: use of percutaneous atherectomy in 579 lesions. Ann Surg. 2008;248(4):519-528. doi:10.1097/SLA.0b013e318188e1de
34. Milnerowicz A, Milnerowicz A, Kuliczkowski W, Protasiewicz M. Rotational atherectomy plus drug-coated balloon angioplasty for the treatment of total in-stent occlusions in iliac and infrainguinal arteries. J Endovasc Ther. 2019;26(3):316-321. doi:10.1177/1526602819836749
35. Ponukumati AS, Suckow BD, Powell CJ, et al. Outcomes of rotational atherectomy in complex lesions of the superficial femoral artery. J Vasc Surg. 2021;73(1):172-178. doi:10.1016/j.jvs.2020.03.040
36. Rastan A, Brodmann M, Böhme T, et al. Atherectomy and drug-coated balloon angioplasty for the treatment of long infrapopliteal lesions: a randomized controlled trial. Circ Cardiovasc Interv. 2021;14(6):e010280. doi:10.1161/CIRCINTERVENTIONS.120.010280
37. Norberto EM, Revilla A, Brizuela JA, Díez M, Taylor JH, Riera Del Moral LF. Directional atherectomy with antirestenotic therapy versus pta/supera stenting for popliteal artery lesions: a propensity-matched analysis. J Endovasc Ther. 2025:32(4):1027-1037. doi:10.1177/15266028231199923
38. Sanon O, Carnevale M, Indes J, Gao Q, Lipsitz E, Koleilat I. Incidence of procedure-related complications in patients treated with atherectomy in the femoropopliteal and tibial vessels in the vascular quality initiative. J Endovasc Ther. 2023;30(5):693-702. doi:10.1177/15266028221091900
39. Savader SJ, Venbrux AC, Mitchell SE, et al. Percutaneous transluminal atherectomy of the superficial femoral and popliteal arteries: long-term results in 48 patients. Cardiovasc Intervent Radiol. 1994;17(6):312-318. doi:10.1007/BF00203949
40. Schöfthaler C, Troisi N, Torsello G, et al. Safety and effectiveness of the Phoenix atherectomy device for endovascular treatment of common femoral and popliteal arteries: results of the EN-MOBILE trial. Vasc Med. 2024;29(4):405-415. doi:10.1177/1358863X241231943
41. Semaan E, Hamburg N, Nasr W, et al. Endovascular management of the popliteal artery: comparison of atherectomy and angioplasty. Vasc Endovascular Surg. 2010;44(1):25-31. doi:10.1177/1538574409345028
42. Siracuse JJ, Gill HL, Cassidy SP, et al. Endovascular treatment of lesions in the below-knee popliteal artery. J Vasc Surg. 2014;60(2):356-361. doi:10.1016/j.jvs.2014.02.012
44. Troisi N, Saratzis A, Katsogridakis E, et al; EMO-POP Registry Collaborative Group. Different endovascular modalities of treatment for isolated atherosclerotic popliteal artery lesions (EMO-POP) registry. J Vasc Surg. 2023;77(1):231-240.e4. doi:10.1016/j.jvs.2022.07.170
45. van den Berg JC, Pedrotti M, Canevascini R, Chimchila Chevili S, Giovannacci L, Rosso R. In-stent restenosis: mid-term results of debulking using excimer laser and drug-eluting balloons: sustained benefit? J Invasive Cardiol. 2014;26(7):333-337.
46. Wei L, Guo J, Guo L, et al. Directional atherectomy and drug-coated balloon angioplasty vs. bare nitinol stent angioplasty for femoropopliteal artery lesions. Vasa. 2022;51(5):275-281. doi:10.1024/0301-1526/a001010
47. Yamamoto Y, Kawarada O, Ando H, et al. Effects of high-speed rotational atherectomy in peripheral artery disease patients with calcified lesions: a retrospective multicenter registry. Cardiovasc Interv Ther. 2020;35(4):393-397. doi:10.1007/s12928-020-00643-9
48. Yang L, Quan J, Dong J, et al. Comparison of mid-outcome among bare metal stent, atherectomy with or without drug-coated balloon angioplasty for femoropopliteal arterial occlusion. Sci Rep. 2024;14(1):63. doi:10.1038/s41598-023-50511-8
49. Yue Y, Zhang Y, Zhang L, Gao Z, Du X, Ran F. Study on mid-term outcomes of atherectomy for patients with femoral popliteal artery lesions with different Global Limb Anatomic Staging System grades. PeerJ. 2024;12:e18189. doi:10.7717/peerj.18189
50. Zeller T, Sixt S, Schwarzwälder U, et al. Two-year results after directional atherectomy of infrapopliteal arteries with the SilverHawk device. J Endovasc Ther. 2007;14(2):232-240. doi:10.1177/152660280701400216
51. Zeller T, Giannopoulous S, Brodmann M, et al. Orbital atherectomy prior to drug-coated balloon angioplasty in calcified infrapopliteal lesions: a randomized, multicenter pilot study. J Endovasc Ther. 2022;29(6):874-884. doi:10.1177/15266028211070968
All CLTI Cohort (N = 25 papers)
1. Bracale UM, Vitale G, Bajardi G, et al. Use of the directional atherectomy for the treatment of femoro-popliteal lesions in patients with critical lower limb ischemia. Transl Med UniSa. 2016;15:42-47.
2. Gandini R, Del Giudice C, Merolla S, Morosetti D, Pampana E, Simonetti G. Treatment of chronic SFA in-stent occlusion with combined laser atherectomy and drug-eluting balloon angioplasty in patients with critical limb ischemia: a single-center, prospective, randomized study. J Endovasc Ther. 2013;20(6):805-814. doi:10.1583/13-4308MR.1
3. Gordon IL, Masukawa K, Williams RA, Wilson SE. Initial results with atherectomy for non-reconstructable limb threatening peripheral vascular disease. Journal of Experimental & Clinical Medicine. 2010;2(6):302-304. doi:10.1016/j.jecm.2010.09.002
4. Kandzari DE, Kiesz RS, Allie D, et al. Procedural and clinical outcomes with catheter-based plaque excision in critical limb ischemia. J Endovasc Ther. 2006;13(1):12-22. doi:10.1583/05-1634.1
5. Kokkinidis DG, Giannopoulos S, Jawaid O, Cantu D, Singh GD, Armstrong EJ. Laser atherectomy for infrapopliteal lesions in patients with critical limb ischemia. Cardiovasc Revasc Med. 2021;23:79-83. doi:10.1016/j.carrev.2020.08.041
6. Laird JR, Zeller T, Gray BH, et al; LACI Investigators. Limb salvage following laser-assisted angioplasty for critical limb ischemia: results of the LACI multicenter trial. J Endovasc Ther. 2006;13(1):1-11. doi:10.1583/05-1674.1
7. Loor G, Skelly CL, Wahlgren C, et al. Is atherectomy the best first-line therapy for limb salvage in patients with critical limb ischemia? Vasc Endovascular Surg. 2009;43(6):542-550. doi:10.1177/1538574409334825
8. Massmann A, Katoh M, Shayesteh-Kheslat R, Buecker A. Mechanical recanalization of subacute vessel occlusion in peripheral arterial disease with a directional atherectomy catheter. Cardiovasc Intervent Radiol. 2012;35(5):1201-1204. doi:10.1007/s00270-012-0364-6
9. McKinsey JF, Zeller T, Rocha-Singh KJ, Jaff MR, Garcia LA, DEFINITIVE LE Investigators. Lower extremity revascularization using directional atherectomy: 12-month prospective results of the DEFINITIVE LE study. JACC Cardiovasc Interv. 2014;7(8):923-933. doi:10.1016/j.jcin.2014.05.006
10. Morosetti D, Chiocchi M, Argiro R, et al. Endovascular treatment of calcific lesions of the common femoral artery using atherectomy device associated with scoring balloon angioplasty in diabetic patients with high “major amputation” risk. Vascular. 2022;30(3):463-473. doi:10.1177/17085381211019244
11. Mustapha JA, Katzen BT, Neville RF, et al. Propensity score-adjusted comparison of long-term outcomes among revascularization strategies for critical limb ischemia. Circ Cardiovasc Interv. 2019;12(9):e008097. doi:10.1161/CIRCINTERVENTIONS.119.008097
12. Palena LM, Saad PF, Piccolo E, et al. Below-the-ankle orbital atherectomy in chronic limb-threatening ischemia patients as a bailout strategy for limb salvage: early clinical experience. Cardiovasc Revasc Med. 2022;42:121-126. doi:10.1016/j.carrev.2022.03.015
13. Pitoulias AG, Taneva GT, Avranas K, Bakr NA, Pitoulias GA, Donas KP. Use of rotational atherectomy-assisted balloon angioplasty in the treatment of isolated below-the-knee atherosclerotic lesions in patients with chronic limb-threatening ischemia. J Clin Med. 2024;13(5):1346. doi:10.3390/jcm13051346
14. Proczka MS, Gałązka Z, Janiszewska M, Ricotta JJ, Ricotta JJ 2nd. Midterm results of atherectomy as an adjunct to endovascular intervention in a population with chronic limb-threatening ischemia. Postepy Kardiol Interwencyjnej.2024;20(3):345-352. doi:10.5114/aic.2024.142494
15. Serino F, Cao Y, Renzi C, et al. Excimer laser ablation in the treatment of total chronic obstructions in critical limb ischaemia in diabetic patients. Sustained efficacy of plaque recanalisation in mid-term results. Eur J Vasc Endovasc Surg. 2010;39(2):234-238. doi:10.1016/j.ejvs.2009.10.018
16. Shammas NW, Lam R, Mustapha J, et al. Comparison of orbital atherectomy plus balloon angioplasty vs. balloon angioplasty alone in patients with critical limb ischemia: results of the CALCIUM 360 randomized pilot trial. J Endovasc Ther. 2012;19(4):480-488. doi:10.1583/JEVT-12-3815MR.1
17. Shammas NW, Yates T, Sastry A, et al. Prospective, Multi-center, single-arm study of the Auryon laser system for treatment of below-the-knee arteries in patients with chronic limb-threatening ischemia: 30-day results of the Auryon BTK. Am J Cardiol. 2024;219:1-8. doi:10.1016/j.amjcard.2024.03.008
18. Sultan S, Tawfick W, Hynes N. Cool excimer laser-assisted angioplasty (CELA) and tibial balloon angioplasty (TBA) in management of infragenicular arterial occlusion in critical lower limb ischemia (CLI). Vasc Endovascular Surg. 2013;47(3):179-191. doi:10.1177/1538574413478473
19. Sumner J, Patel S, Theodoulou I, et al. Combined treatment of native femoropopliteal occlusions in chronic limb-threatening ischemia using atherectomy debulking and a new sirolimus drug-coated balloon (SELUTION SLR). The Arab Journal of Interventional Radiology. 2024;8(2):70-77. doi:10.1055/s-0044-1782664
20. Tan T, Semaan E, Nasr W, et al. Endovascular revascularization of symptomatic infrapopliteal arteriosclerotic occlusive disease: comparison of atherectomy and angioplasty. Int J Angiol. 2011;20(1):19-24. doi:10.1055/s-0031-1272545
21. Todd KE Jr, Ahanchi SS, Maurer CA, Kim JH, Chipman CR, Panneton JM. Atherectomy offers no benefits over balloon angioplasty in tibial interventions for critical limb ischemia. J Vasc Surg. 2013;58(4):941-948. doi:10.1016/j.jvs.2013.04.024
22. Yancey AE, Minion DJ, Rodriguez C, Patterson DE, Endean ED. Peripheral atherectomy in TransAtlantic InterSociety Consensus type C femoropopliteal lesions for limb salvage. J Vasc Surg. 2006;44(3):503-509. doi:10.1016/j.jvs.2006.05.038
23. Yang S, Li S, Hou L, He J. Excimer laser atherectomy combined with drug-coated balloon versus drug-eluting balloon angioplasty for the treatment of infrapopliteal arterial revascularization in ischemic diabetic foot: 24-month outcomes. Lasers Med Sci. 2022;37(3):1531-1537. doi:10.1007/s10103-021-03393-z
24. Yang Y, Lin T, Chou C, et al. Effect of limb salvage by excimer laser angioplasty plus low-pressure balloon inflation in chronic limb-threatening ischemia patients with infrapopliteal vessel disease. Acta Cardiol Sin. 2023;39(5):765-772. doi:10.6515/ACS.202309_39(5).20230115A
25. Zia S, Juneja A, Shams S, et al. Contemporary outcomes of infrapopliteal atherectomy with angioplasty versus balloon angioplasty alone for critical limb ischemia. J Vasc Surg. 2020;71(6):2056-2064. doi:10.1016/j.jvs.2019.08.254
43. Stoner MC, deFreitas DJ, Phade SV, Parker FM, Bogey WM, Powell S. Mid-term results with laser atherectomy in the treatment of infrainguinal occlusive disease. J Vasc Surg. 2007;46(2):289-295. doi:10.1016/j.jvs.2007.04.019
References
1. Abu Dabrh AM, Steffen MW, Undavalli C, et al. The natural history of untreated severe or critical limb ischemia. J Vasc Surg. 2015;62(6):1642-1651.e3. doi:10.1016/j.jvs.2015.07.065
2. Writing Committee Members; Gornik HL, Aronow HD, Goodney PP, et al. 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline for the Management of Lower Extremity Peripheral Artery Disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2024;83(24):2497-2604. doi:10.1016/j.jacc.2024.02.013
3. Conte MS, Bradbury AW, Kolh P, et al; GVG Writing Group. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019;69(6S):3S-125S.e40. doi:10.1016/j.jvs.2019.02.016
4. Aboyans V, Ricco J, Bartelink MEL, et al; ESC Scientific Document Group. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries. Endorsed by: the European Stroke Organization (ESO), The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018;39(9):763-816. doi:10.1093/eurheartj/ehx095
5. Bradbury AW, Moakes CA, Popplewell M, et al; BASIL-2 Investigators. A vein bypass first versus a best endovascular treatment first revascularisation strategy for patients with chronic limb threatening ischaemia who required an infra-popliteal, with or without an additional more proximal infra-inguinal revascularisation procedure to restore limb perfusion (BASIL-2): an open-label, randomised, multicentre, phase 3 trial. Lancet. 2023;401(10390):1798-1809. doi:10.1016/S0140-6736(23)00462-2
6. Fanelli F, Cannavale A, Gazzetti M, et al. Calcium burden assessment and impact on drug-eluting balloons in peripheral arterial disease. Cardiovasc Intervent Radiol. 2014;37(4):898-907. doi:10.1007/s00270-014-0904-3
7. Reijnen MMPJ, van Wijck I, Brodmann M, et al; IN.PACT Global Study Investigators. Five-year outcomes after paclitaxel drug-coated balloon treatment of femoropopliteal lesions in diabetic and chronic limb-threatening ischemia cohorts: IN.PACT global study post hoc analysis. Cardiovasc Intervent Radiol. 2023;46(10):1329-1345. doi:10.1007/s00270-023-03478-y
8. Zettervall SL, Marshall AP, Fleser P, Guzman RJ. Association of arterial calcification with chronic limb ischemia in patients with peripheral artery disease. J Vasc Surg. 2018;67(2):507-513. doi:10.1016/j.jvs.2017.06.086
9. Shammas NW, Coiner D, Shammas G, Jerin M. Predictors of provisional stenting in patients undergoing lower extremity arterial interventions. Int J Angiol. 2011;20(2):95-100. doi:10.1055/s-0031-1279683
10. Tepe G, Beschorner U, Ruether C, et al. Drug-eluting balloon therapy for femoropopliteal occlusive disease: predictors of outcome with a special emphasis on calcium. J Endovasc Ther. 2015;22(5):727-733. doi:10.1177/1526602815600156
11. Chowdhury M, Secemsky EA. Atherectomy vs other modalities for treatment during peripheral vascular intervention. Curr Cardiol Rep. 2022;24(7):869-877. doi:10.1007/s11886-022-01709-1
12. Wardle BG, Ambler GK, Radwan RW, Hinchliffe RJ, Twine CP. Atherectomy for peripheral arterial disease. Cochrane Database Syst Rev. 2020;9(9):CD006680. doi:10.1002/14651858.CD006680.pub3
13. Pan D, Guo J, Su Z, et al. Efficacy and safety of atherectomy combined with balloon angioplasty vs balloon angioplasty alone in patients with femoro-popliteal lesions: a systematic review and meta-analysis of randomized controlled trials. J Endovasc Ther. 2025;32(5):1326-1338. doi:10.1177/15266028231215354
14. Wu Z, Huang Q, Pu H, et al. Atherectomy combined with balloon angioplasty versus balloon angioplasty alone for de novo femoropopliteal arterial diseases: a systematic review and meta-analysis of randomised controlled trials. Eur J Vasc Endovasc Surg. 2021;62(1):65-73. doi:10.1016/j.ejvs.2021.02.012
15. Wu H, Zheng D, Zhou L, Wang Q, Wang T, Liang S. A systematic review and meta-analysis of atherectomy plus balloon angioplasty versus balloon angioplasty alone for infrapopliteal arterial disease. J Endovasc Ther. 2025;32(4):957-968. doi:10.1177/15266028231209236
16. Nagarsheth KH, Jreij G, Saab F. A systematic review of clinical trials in patients with critical limb-threatening ischemia. J Crit Limb Ischem. 2025;5(2):E29-E35. doi:10.25270/jcli/CLIG-2400010
17. Carr JG, Langhoff R, DeRubertis BG, et al. Published evidence on peripheral atherectomy: a meta-analysis and systematic literature review of more than 300 original investigations. J Soc Cardiovasc Angiogr Interv. 2025;4(11):104009. doi:10.1016/j.jscai.2025.104009
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
19. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. doi:10.1001/jama.283.15.2008
20. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153-160. doi:10.1136/ebmental-2019-300117
21. Higgins JPT, Thomas J, Chandler J, et al, eds. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5, August 2024. Cochrane; 2024.
22. The R Foundation. The R Project for Statistical Computing. https://www.R-project.org. Accessed March 31, 2025.
23. Noory E, Böhme T, Steinhauser Y, et al. Acute and mid-term results of atherectomy in femoropopliteal lesions. J Endovasc Ther. 2025;32(6):2137-2146. doi:10.1177/15266028241240898
24. Zeller T, Langhoff R, Rocha-Singh KJ, et al; DEFINITIVE AR Investigators. Directional atherectomy followed by a paclitaxel-coated balloon to inhibit restenosis and maintain vessel patency: twelve-month results of the DEFINITIVE AR study. Circ Cardiovasc Interv. 2017;10(9):e004848. doi:10.1161/CIRCINTERVENTIONS.116.004848
25. Dave RM, Patlola R, Kollmeyer K, et al. Excimer laser recanalization of femoropopliteal lesions and 1-year patency: results of the CELLO registry. J Endovasc Ther. 2009;16(6):665-675. doi:10.1583/09-2781.1
26. McKinsey JF, Zeller T, Rocha-Singh KJ, Jaff MR, Garcia LA, DEFINITIVE LE Investigators. Lower extremity revascularization using directional atherectomy: 12-month prospective results of the DEFINITIVE LE study. JACC Cardiovasc Interv. 2014;7(8):923-933. doi:10.1016/j.jcin.2014.05.006
27. Babaev A, Zavlunova S, Attubato MJ, Martinsen BJ, Mintz GS, Maehara A. Orbital atherectomy plaque modification assessment of the femoropopliteal artery via intravascular ultrasound (TRUTH Study). Vasc Endovascular Surg. 2015;49(7):188-194. doi:10.1177/1538574415607361
28. Rastan A, McKinsey JF, Garcia LA, et al; DEFINITIVE LE Investigators. One-year outcomes following directional atherectomy of infrapopliteal artery lesions: subgroup results of the prospective, multicenter DEFINITIVE LE trial. J Endovasc Ther. 2015;22(6):839-846. doi:10.1177/1526602815608610
29. Mustapha JA, Finton SM, Diaz-Sandoval LJ, Saab FA, Miller LE. Percutaneous transluminal angioplasty in patients with infrapopliteal arterial disease: systematic review and meta-analysis. Circ Cardiovasc Interv. 2016;9(5):e003468. doi:10.1161/CIRCINTERVENTIONS.115.003468
30. Mustapha JA, Igyarto Z, O’Connor D, et al. One-year outcomes of peripheral endovascular device intervention in critical limb ischemia patients: sub-analysis of the LIBERTY 360 study. Vasc Health Risk Manag. 2020;16:57-66. doi:10.2147/vhrm.S230934
31. Almasri J, Adusumalli J, Asi N, et al. A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia. J Vasc Surg. 2019;69(6S):126S-136S. doi:10.1016/j.jvs.2018.01.071
32. Reijnen MMPJ, van Wijck I, Zeller T, et al. Outcomes after drug-coated balloon treatment of femoropopliteal lesions in patients with critical limb ischemia: a post hoc analysis from the IN.PACT global study. J Endovasc Ther. 2019;26(3):305-315. doi:10.1177/1526602819839044
33. Gandini R, Del Giudice C, Merolla S, Morosetti D, Pampana E, Simonetti G. Treatment of chronic SFA in-stent occlusion with combined laser atherectomy and drug-eluting balloon angioplasty in patients with critical limb ischemia: a single-center, prospective, randomized study. J Endovasc Ther. 2013;20(6):805-814. doi:10.1583/13-4308MR.1
34. Massmann A, Katoh M, Shayesteh-Kheslat R, Buecker A. Mechanical recanalization of subacute vessel occlusion in peripheral arterial disease with a directional atherectomy catheter. Cardiovasc Intervent Radiol. 2012;35(5):1201-1204. doi:10.1007/s00270-012-0364-6
35. Morosetti D, Chiocchi M, Argiro R, et al. Endovascular treatment of calcific lesions of the common femoral artery using atherectomy device associated with scoring balloon angioplasty in diabetic patients with high “major amputation” risk. Vascular. 2022;30(3):463-473. doi:10.1177/17085381211019244
36. Shammas NW, Lam R, Mustapha J, et al. Comparison of orbital atherectomy plus balloon angioplasty vs. balloon angioplasty alone in patients with critical limb ischemia: results of the CALCIUM 360 randomized pilot trial. J Endovasc Ther. 2012;19(4):480-488. doi:10.1583/JEVT-12-3815MR.1
37. Bath J, Lawrence PF, Neal D, et al. Endovascular interventions for claudication do not meet minimum standards for the Society for Vascular Surgery efficacy guidelines. J Vasc Surg. 2021;73(5):1693-1700.e3. doi:10.1016/j.jvs.2020.10.067
38. Mukherjee D, Contos B, Emery E, Collins DT, Black JH, 3rd. High reintervention and amputation rates after outpatient atherectomy for claudication. Vasc Endovascular Surg. 2018;52(6):427-433. doi:10.1177/1538574418772459
39. Kawaji Q, Dun C, Walsh C, et al. Index atherectomy peripheral vascular interventions performed for claudication are associated with more reinterventions than nonatherectomy interventions. J Vasc Surg. 2022;76(2):489-498.e4. doi:10.1016/j.jvs.2022.02.034
40. Mustapha JA, Katzen BT, Neville RF, et al. Propensity score-adjusted comparison of long-term outcomes among revascularization strategies for critical limb ischemia. Circ Cardiovasc Interv. 2019;12(9):e008097. doi:10.1161/CIRCINTERVENTIONS.119.008097
41. Giannopoulos S, Ghanian S, Parikh SA, Secemsky EA, Schneider PA, Armstrong EJ. Safety and efficacy of drug-coated balloon angioplasty for the treatment of chronic limb-threatening ischemia: a systematic review and meta-analysis. J Endovasc Ther. 2020;27(4):647-657. doi:10.1177/1526602820931559
42. Farber A, Menard MT, Conte MS, et al; BEST-CLI Investigators. Surgery or endovascular therapy for chronic limb-threatening ischemia. N Engl J Med. 2022;387(25):2305-2316. doi:10.1056/NEJMoa2207899
43. Al Halabi S, Templeton E, Heaney C, et al. Drug-coated versus uncoated percutaneous transluminal angioplasty balloons for the treatment of infrapopliteal peripheral artery disease: a systematic review and meta-analysis of randomized controlled trials. J Crit Limb Ischem. 2022;2(1):E11-E16.
44. Caradu C, Lakhlifi E, Colacchio EC, et al. Systematic review and updated meta-analysis of the use of drug-coated balloon angioplasty versus plain old balloon angioplasty for femoropopliteal arterial disease. J Vasc Surg. 2019;70(3):981-995.e10. doi:10.1016/j.jvs.2019.01.080